Medical Psychology and Sociology: Emotions
Are you able to name the six basic human emotions? Happiness, sadness, anger, fear, surprise, and disgust. How do emotions arise and how can they be measured? What anatomic correlations should you know? What are the most important theories about emotions? The following article answers all of these and even more questions. Moreover, you will learn important clinical connections: anxiety disorders and depression are common diseases that you will encounter in your clinical routine. Make yourself familiar with the basics so that you are perfectly prepared for preclinical exams and your "Physikum".
Table of Contents
Are you more of a visual learner? Check out our online video lectures and start your psychology and sociology course now for free!

Definition and Components of Emotion
Definition: An emotion is a subjective, important human reaction to a physical stimulus. Situations, actions, or concrete objects can have negative or positive meanings for individuals.
The three components of the hypothetical construct emotion
- Physiological component
- Cognitive component
- Behavioral component: expression (facial expressions/gestures) and motivation
 Physiological arousal refers to the excitation of the body´s internal state. Behavioral reactions to emotion include some expressive behavior. Cognitive aspect involves an appraisal or interpretation of the situation.
Physiological arousal refers to the excitation of the body´s internal state. Behavioral reactions to emotion include some expressive behavior. Cognitive aspect involves an appraisal or interpretation of the situation.Darwin assumed that emotions had a strong biological basis. He argued that they evolved via natural selection and have universal cross-cultural expression. This has been validated and supported by preliterate cultures. There are six major universal emotions.
Distinction of the terms feeling, mood, and affect from emotion
- Feeling: subjective affective component, average duration, and average intensity
- Mood: longer duration, less intense
- Affect: very short, severe wave of emotion (“murder in the heat of the moment”)
Adaptive role of emotion
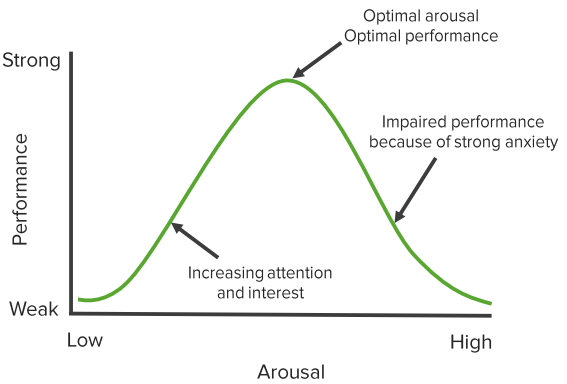 The Yerkes-Dodson Law states that the relationship between performance and emotional arousal is a U-shaped correlation. There is an “optimal” range where arousal provides benefit, varies by individual.
The Yerkes-Dodson Law states that the relationship between performance and emotional arousal is a U-shaped correlation. There is an “optimal” range where arousal provides benefit, varies by individual.Emotion may enhance survival by increasing arousal and priming for quick decisions (fear, anger). Emotions can influence daily life decisions providing framework and consequences.
Theories of emotion
James-Lange Theory- Physiological and behavioral responses to a stimuli trigger the cognitive aspect of emotion
- Support includes effects of smiling and shallow vs. deep breaths
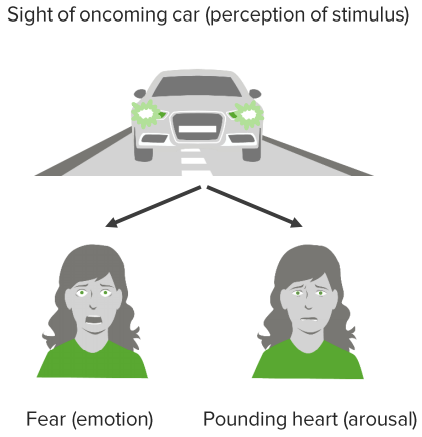
 | Fight or flight |  |
| Perception of emotion — arousing stimulus | Specific physiological changes | Interpretation of physiological changes as the emotion |
- Each emotion originates from a distinctive physiological state. Many emotional states share similar physiological patterns (i.e. fear and sexual arousal).
- Assumption that we possess the ability to label physiological states accurately. Physiological states can be interpreted differently based on context (i.e. anxiety vs. excitement).

Cannon-Bard Theory
 Physiological and cognitive responses to a stimuli occur simultaneously and independently. This then leads to a behavioral reaction. This model is able to explain the overlap in physiological states between emotions (i.e. fear and sexual arousal). It is unable to explain the phenomenon in which behavioral response influences the physical and cognitive aspects of emotion (i.e. smiling leads to happiness).
Physiological and cognitive responses to a stimuli occur simultaneously and independently. This then leads to a behavioral reaction. This model is able to explain the overlap in physiological states between emotions (i.e. fear and sexual arousal). It is unable to explain the phenomenon in which behavioral response influences the physical and cognitive aspects of emotion (i.e. smiling leads to happiness).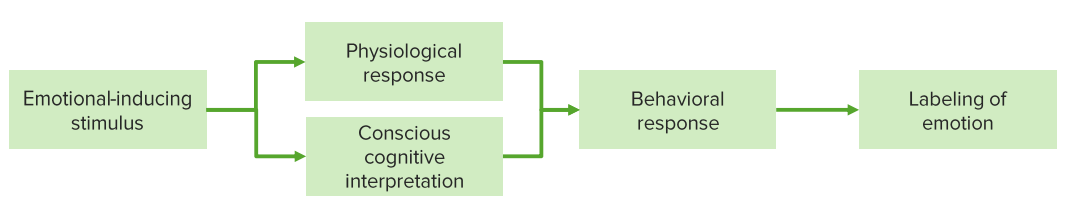
Schachter-Singer Theories of emotion
Physiological arousal leads to conscious cognitive interpretation based on circumstance.

Summary
| James and Lange’s Theory “We don’t cry because we are sad, we are sad because we cry.” | Physical changes are the reason for emotions. Pattern: Perception of the object – triggering of physical reactions – perception as emotion |
| Cannon and Bard’s Theory | Emotions are only possible via perception of stimuli/perception of stimuli in the brain. Pattern: Perception of the object – activation of thalamus – simultaneous physiological and emotional excitation (preprogrammed reflex) |
| Schachter and Singer’s Two-Components Theory “No emotion without cognition.” | The precondition for emotion is an unspecific physiological stimulus. Pattern: Stimulus – unspecific physiological excitement – cognitive assessment – emotion |
Classification of Emotions
Emotions are classified into primary emotions and secondary emotions. Current scientific knowledge estimates the first development of primary emotions to be of genetic origin.The six primary emotions
- Happiness
- Sadness
- Anger
- Fear
- Surprise
- Disgust
Secondary emotions: Blended emotions or “learned” emotions
To a large extent, genetics may be responsible for the development of primary emotions. However, social and cultural influences shape the subsequent experience of emotions.A culturally specific example is the appropriateness of emotions in certain situations. Anger is either unleashed in rage or controlled. Social roles shape emotional behavior even further. Boys are for example still taught that crying is not appropriate behavior for men.
Measuring Emotions: Quality and Intensity
Qualitative dimensions of measuring emotions (by W. Wundt)
- Desire-displeasure
- Excitement-calm
- Tension-relaxation
Psychophysiological methods
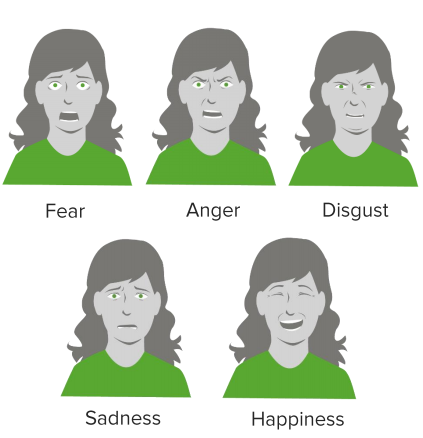
Emotions can be measured by means of muscle activity. The FACS makes a classification possible.Ekman and Friesen’s classification of basic emotions and facial expressions (1978)
| Basic emotion | Facial expression |
| Happiness | Tense lower eyelid raised corners of the mouth |
| Surprise | Raised eyebrows, raised upper eyelid, opened mouth |
| Anger | Lowered eyebrows, frowning, raised upper eyelid, tense lower eyelid |
| Disgust | Tense lower eyelid raised upper lip |
| Fear | Partly raised/partly lowered eyebrows, frowning, raised upper eyelid, opened mouth |
| Sadness | Partly raised/partly lowered eyebrows, lowered corner of the mouth |
| Disdain | Tense corner of the mouth raised on one side |
Neurobiological Basics of Emotions
Below we will present you with the anatomically important correlates for the generation and processing of emotions.- Parasympathetic and sympathetic nervous system: Control of the physiological components via catecholamines (noradrenaline and adrenaline).
- Frontal lobe: Lesions in this cerebral area lead to disorders of social behavior: social interaction becomes only possible in a reduced or inappropriate way. Facial expressions and gestures are also diminished by the frontal lobe (poker face).
- Hypothalamus and limbic system: Controls the release of hormones and neurotransmitters. (The limbic system is named after P. Broca “Ia grande lobe limbique” and is not an anatomical but a functional unit for emotion, drive, and learning.).
- Amygdalae: If the amygdalae are removed on both sides, fear is reduced and otherwise dangerous stimuli are no longer perceived as aversive. Without the amygdalae, there is no fight-or-flight reaction to conditioned fear stimuli.
- Hippocampus: Responsible for comparing expectations and actual sensory information. Mismatches are opposed by a behavior-stop-system. Without the hippocampus, vital avoidance behavior is severely impaired.
Fear as Emotion
Fear has many qualities. Roughly speaking it describes the feeling of being threatened and of anxiety. The different above-mentioned components usually express themselves (even though there are great differences from one person to another!) as follows:| Physiological component | Cognitive component | Observable behavior |
| Tachycardia, tremor, chills, nausea, urge to urinate | Worries, speculation, concern | Raising of the lower lip, tension of eyelids |
Although the complete lack of fear may be desirable at first glance, it leaves the affected person without any of the very important protective effects.
Other types of fear:- Concrete fear: emotional, appropriate fear reaction (anxiety)
- Phobia: exaggerated reaction to a certain situation (objects like spiders = arachnophobia)
State anxiety vs. trait anxiety
| STATE | TRAIT |
| Acute, situational state of fear | Long-lasting personal characteristic, disposition that is stable over time |
Sensitizer or repressor?
Do you deal with your fear deliberately or do you repress or suppress your fear as best as possible?Sensitizers try to gather as much information as possible about the situation, the object or the circumstances that frighten them (e.g. the package information for drugs is read in great detail).
Repressors try to expose themselves as little as possible to factors that trigger fear. Both behaviors are possible means to cope with fear.
Practical advice: As a physician, you have to learn to handle both types of coping with fear. Conversations and therapies have to be customized according to the coping strategy and the patient’s wish for information (e.g. does the patient want information about every little detail of a routine surgery or does he want only basic information?).
Anxiety disorders: Neuroses
Generalized anxiety disorder
Affected individuals suffer from diffuse fear and are permanently tense, brooding, worried and full of concern about trivial things.Panic disorder
A panic disorder is diagnosed when patients spontaneously, as if “struck by thunder” in their everyday lives, suffer from panic attacks. The affected individuals are severely impaired! Often physicians do not detect panic disorders because of the use of exclusion diagnostics only.Specific phobias
In the case of specific phobias, fears and respective avoidance strategies focus on a specific object or situation. A few common examples that quite frequently occur in exam questions are the following:- Phobia of animals like arachnophobia (fear of spiders) or cynophobia (fear of dogs)
- Hemophobia (fear of blood)
- Aviophobia(fear of flying)
- Acrophobia (fear of heights)
- Claustrophobia (fear of narrow, closed rooms or spaces)
Social phobias
Social phobias describe the fear of social situations in which one could disgrace oneself or be humiliated. They are characterized by a fear of being assessed negatively by others in interaction and performance situations.Agoraphobia
People suffering from agoraphobia are afraid of public places, crowds, and means of transport as well as other situations where an escape could be difficult or embarrassing. Agoraphobia has a high comorbidity with panic disorders.Obsessive-compulsive disorders
Obsessive-compulsive disorders are based on fear as well. Patients suffering from compulsions are afraid that terrible things are going to happen if they cannot carry out the compulsive act (“If I do not tie my shoelaces seven times my grandfather will die.”). Usually, the compulsive acts consume most of the day and impair the patient’s quality of life significantly.The most common obsessions are:
- Washing obsession
- Control obsession (e.g. continuous checking of electronic devices in the apartment)
Aggression as Emotion: Instinct or Learned?
Definition: Motive to harm oneself (self-harm) or others
The development of aggression – three possible explanations
Psychoanalytical perspectiveAccording to psychoanalytic theory, Thanatos, the death instinct, is responsible for aggression. Human beings are compared to “steam boilers” that build up the pressure until the pressure has to be released.
Aggressive venting is a purification process (catharsis hypothesis) that reduces drive tension. It is assumed that, for example, the viewing of aggressive scenes of a film substitutes for the real release of aggression. This view contradicts the theory, that the original form of aggressive behavior is learned!
Ethological perspective
Ethology interprets aggression as an animalistic instinct that serves the defense of habitat, the protection of the community, and the creation/preservation of social hierarchy.
Learned behavior-perspective
This theory is based on the assumption that aggressive behavior is acquired through theoretical learning mechanisms. Special emphasis is placed on learning from role models.
Dollard and Miller’s frustration-aggression hypothesis (1950)
The frustration-aggression hypothesis has its focus on the conditions that are responsible for the development of aggression. Frustration is experienced if an aspired goal is not reached because external factors act as obstacles.
People with high frustration tolerance are better at handling restrictions on their way to achieving a goal and without having their physical and psychological wellbeing offended; hence, they do not need to release tension through aggression.
Depression
 Sadness, shame, disgust, rage, anger, hostility, and fear characterize the feeling of depression, an affective disorder. According to the DSM-IV, at least 4 other symptoms have to be present in addition to a loss of interest or low spirit in order for depression (unipolar disorder/major depression) to be diagnosed.
Sadness, shame, disgust, rage, anger, hostility, and fear characterize the feeling of depression, an affective disorder. According to the DSM-IV, at least 4 other symptoms have to be present in addition to a loss of interest or low spirit in order for depression (unipolar disorder/major depression) to be diagnosed.- Sadness
- Loss of interest
- Feeling of inferiority
- Sleep disorder
- Lethargy/restlessness
- Loss of appetite/increased appetite
- Difficulty concentrating
- Suicidal thoughts
Explanatory models: How does depression develop?
Besides the genetic component (especially in the case of bipolar disorders), neurochemical and environmental factors play a major role. Risk factors that contribute to the risk of developing depression are female gender, serious loss event (divorce, death of important attachment figures, loss of work, etc.) and low socio-economic status.| Model for the development of depression | Example | |
| Lewinsohn’s Loss-of-Reinforcement Theory | Little positive reinforcement in everyday life through:
| Feeling pleasure in baking a cake for oneself and one’s partner. No motivation after separation because the positive reinforcement is missing. |
| Aaron Beck’s Cognitive Explanation | Depression as a consequence of a distorted view of reality: negative evaluation of oneself, the environment and the future (cognitive triad) | “I’m just incapable of a relationship, everybody else thinks that and that’s never going to change.” |
| Seligman’s Learned Helplessness Theory | Basic assumption derived from experimental animal research: lack of avoidance behavior even with missing exposition to pain. Symptoms of learned helplessness:
| Even after rats were unharnessed from the electric shock plate and could have fled to the safe part of the cage, they continued to sit in the danger zone where they were exposed to pain. |
Pain: An Unpleasant Sensory and Emotional Experience
The International Association for the Study of Pain (IASP) defines pain as an “unpleasant sensory- and emotional experience associated with actual or potential tissue damage or described in terms of such damage.”The subjectivity of pain differs greatly between individuals: susceptibility to pain, sensibility to pain, and the relation of pain to its cause vary to a great degree among individuals.
The five components of pain
There are five different components of pain:- Affective: unenthusiastic emotion
- Cognitive-assessing: assessment of the experience of pain
- Motoric: motor reaction to pain
- Sensorial: activity of nociceptors
- Autonomic: reaction of the autonomic nervous system
Important terms to the topic of pain
The sensitivity to pain, which is referred to as algesia, is interrupted in the case of analgesia (medicinally through analgesics).The pain threshold defines the point beyond which a consciously perceived stimulus is perceived as painful.
The point in time when a patient starts taking measures against the pain is his or her intervention threshold. The tolerance threshold is the maximum intensity of pain a person can endure (exceeding this threshold can result in loss of self-control, shock, and coma). Phantom pain is experienced in body parts that have been removed (e.g. after amputations). Phantom pains are explained by the reorganization of the sensory cortex areas. Chronic pain refers to pain that lasts longer than 6 months.
Note: The experience of pain is more intense for people dealing with depression and social isolation than for aged persons and those with reduced vigilance.
Review Questions
The answer key can be found below the references.1. What is the term for severe anxiety attacks that are not related to any specific situational cause and among other symptoms can be accompanied by tachycardia?
- Generalized anxiety disorder
- Cynophobia
- Obsessive-compulsive disorder
- Specific phobia
- Panic disorder
- …the recurring fear of being betrayed and deceived.
- …a generalized anxiety disorder.
- …a specific phobia.
- …a personality-related fear disposition.
- ….situational acute states of fear with tachycardia, nausea, and cold sweat.
- Emotion theory of cognitive assessment
- Cannon and Bard’ Theory
- James and Lange’s Theory
- Schachter and Singer’s Theory
- Two-Components Theory



Comentários
Enviar um comentário