Anatomy of the Upper Limb: Hand Joint
Table of Contents
Surface Anatomy of the Hand Joint
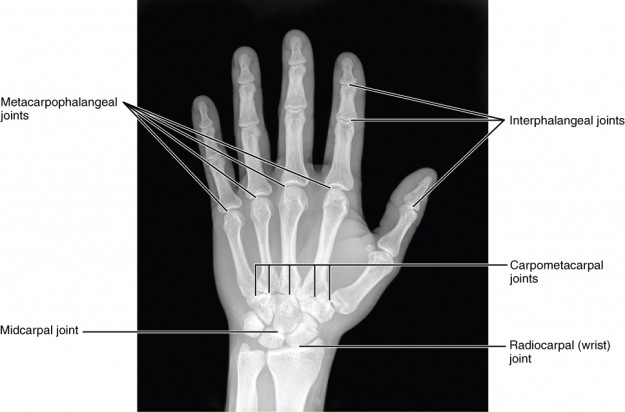
When the hand joint is discussed in human medicine, two sections are being talked about:
- Radiocarpalis (proximal)
- Mediocarpalis (distal)
The hand joint is an extraordinarily mobile joint and moves along a horizontal and sagittal axis. The horizontal axis runs parallel to the slope level of the radius and the caput ossis capitatum.
Dorsal extension and palmar flexion take place around these. The sagittal axis stands vertical to the dorsum manus, passes through the caput ossis capitatum and then runs through the horizontal axis. Radial and ulnar abduction take place along the sagittal axis.
The average active degrees of movement of the hand joint are:
- 80 degrees of dorsal extension
- 80 degrees of palmar flexion
- 20 degrees of radial abduction
- 35 degrees of ulnar abduction
Articulatio Radiocarpalis
The radius and the discus ulnocarpalis articulate with the proximal carpal series and form the art. radiocarpalis, the proximal hand joint. This is an ellipsoidal joint.
Art. radiocarpalis: Osseous structures and joint surfaces of the distal radius

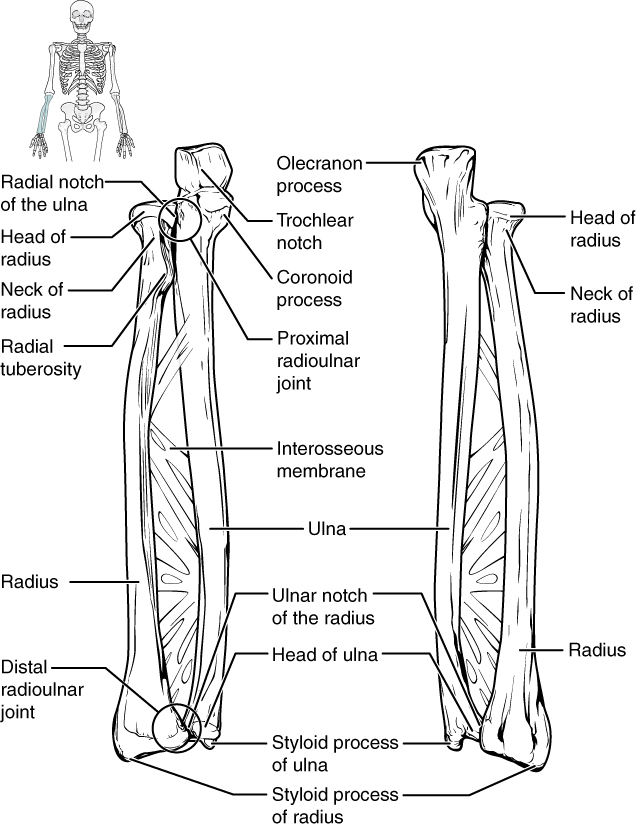
The distal radius has two joint surfaces, one of which is distally oriented, the other ulnar.
The facies articularis carpalis is the joint surface pointing distal and which articulates with the proximal carpal series. It has two concave facets that touch the os scaphoideum and the os lunatum respectively and are designated accordingly: fovea scaphoidea and fovea lunata. Both facets are separated from one another by a cartilage-covered bar. The ulnar-oriented joint surface is the incisura ulnaris, which laterally enters the fovea lunata.
Art. radiocarpalis: Osseous structures and joint surfaces of the distal ulna
The dorsally protruding caput ulnae end in the processus styloideus ulnae. These bony structures have no direct contact with the proximal carpal series, unlike their radial counterparts. This contact crucial for articulation is provided via the discus articularis ulnocarpalis with the os lunatum and the os triquetrum.
Art. radiocarpalis: Discus articularis ulnocarpalis and meniscus ulnocarpalis
Both structures fill the osseous gap between the distal ulna and the proximal carpal series, though they are localized differently despite the small space.
The discus articularis ulnocarpalis is located distal from the ulna and forms the concave surface to the os lunatum and os triquetrum. Its base is located distal to the incisura ulnaris radii and its apex is fastened along the proc. styloideus ulnae and the lig. collaterale carpi ulnare.
The palmar and dorsal edges of the disc are also connate with the joint capsule, which is supposed to prevent dislocation of the disc during terminal motions. It is provided with blood and nutrients via the dorsal and palmar vascular arcade, whereby only the outer layers have direct contact with the vessels. The inner area is avascular and is nourished by pressure and release, similar to the intervertebral discs and menisci of the knee joint.
Between the disc and the os triquetrum is the meniscus ulnocarpalis. It is connate with the ulnar collateral ligament, the palmar side of the os triquetrum and os pisiforme, and slightly connate with the discus articularis ulnocarpalis (proximal segment). It performs the buffer function during movement typical of a meniscus.
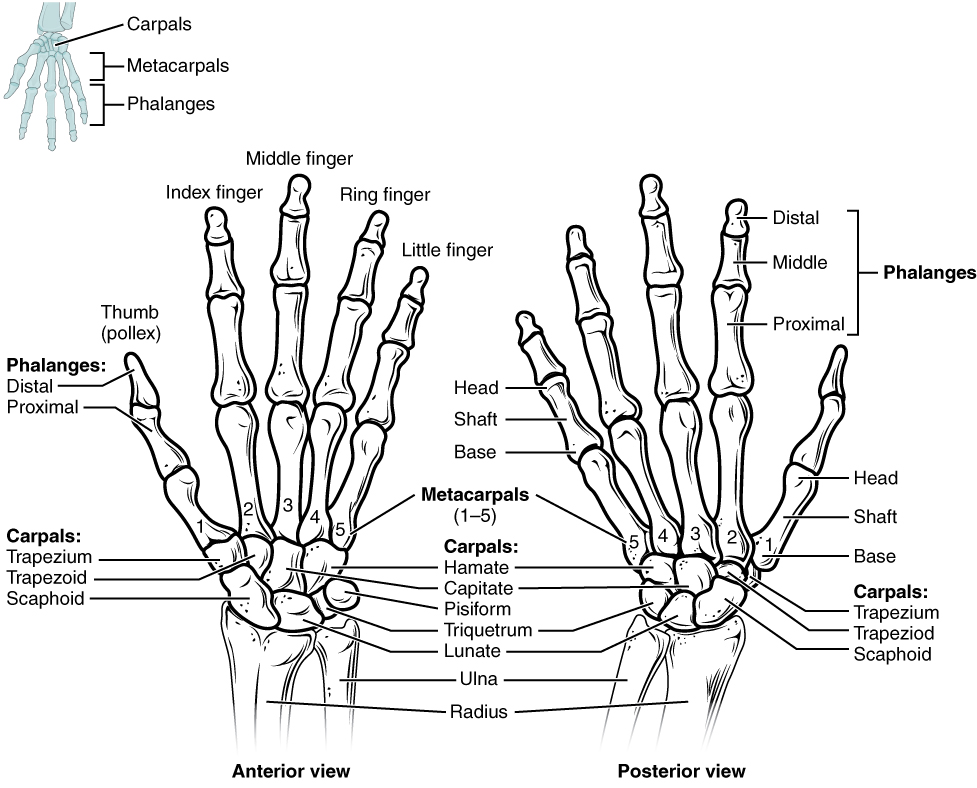
Art. radiocarpalis: Proximal carpal series
Os scaphoideum, os lunatum, and os triquetrum form the distal joint partner of the proximal hand joint.

Image: “wrist- scheme” by Zoph. License: CC BY-SA 3.0 Legende: A – Os scaphoideum, B – Os lunatum, C – Os triquetrum, D – Os pisiforme, E – Os trapezium, F – Os trapezoideum, G – Os capitatum, H – Os hamatum, 1 – Radius, 2 – Ulna, 3 – Ossa metacarpalia
Os scaphoideum
The scaphoid articulates with the radius with its convex joint surface. It has additional ulnar osseous contact with the os lunatum, distal-ulnar with the os capitatum, and distal-radial with the ossa trapezii. The palmar tuberculum scaphoideum is an insertion point for the lig. carpi transversum.
Os lunatum
The os lunatum is a relatively small carpal bone named for its shape, reminiscent of a half moon. Its proximal joint surface is convex and articulates with the fovea lunata radii. Furthermore, it also makes contact with the interosseous disc, the os capitatum, the os scaphoideum and the os triquetrum.
Os triquetrum
The convex os triquetrum only makes contact with the interosseous disc during the ulnar abduction. It also makes contact with the os hamatum and the os pisiforme.
Os pisiforme
The os pisiforme is located directly on top of the os triquetrum and is a sesamoid bone that inserts into the end tendon of the m. flexor carpi ulnaris and its carpal ligament continuations. It also serves as an insertion point and origin for the following structures:
- carpi transversum
- abductor digiti minimi
- collatarale carpi ulnare
- Discus articularis ulnocarpalis
Because of this, the translatability of this bone is very low and only possible in a radial and ulnar direction.
Art. radiocarpalis: Joint capsule
The joint capsule of the proximal hand joints inserts into the bone-cartilage threshold of the proximal carpal series as well as the radius. The disc ulnocarpalis is intracapsular, its end fixation being located in the distal corner of the ulna.
The membrana fibrosa is connected to the palmar and dorsal ligaments and is largely dorsally connate with the synovial tendon sheaths. The capsule also forms a rec. ulnaris between the meniscus and the disc, as well as small palmar and dorsal recesses along the radial side.
Articulatio Mediocarpalis

As the name implies, the distal hand joint makes no articular contact with the ulna and radius, rather solely with the proximal and distal carpal series. The bones of the proximal carpal series are the os scaphoideum, os lunatum, and os triquetrum.
Art. mediocarpalis: Distal carpal series
Those of the distal carpal series is the os trapezium and os trapezoideum (ossa trapezii), and the os capitatum and os hamatum.
Os trapezium
With its concave joint surface, the os trapezium articulates with the os scaphoideum. It also has a flat joint surface to the os trapezoideum and a saddle-shaped joint surface to the basis metacarpale I (thumb).
Ultimately it makes contact with the basis ossis metacarpalis II. The tuberculum ossis trapezii have an osseous groove through which pass the tendons of the m. flexor carpi radialis and which serves as an insertion point for the lig. carpi transversum.
Os trapezoideum
This is the smallest of the carpal bones, with a concave joint surface to the os scaphoideum. It also makes contact with the os capitatum, the os trapezium, and the basis metacarpalis II.
Os capitatum
The os capitatum is one of the largest carpal bones and has a cartilage-coated, convex joint surface to the os scaphoideum and os lunatum. With the basis ossis metacarpalis III it forms the art. carpometacarpale and, with two radial facets, articulates with both the basis ossis metacarpalis II and the os trapezoideum.
Two ulnar facets articulate with the os metacarpale IV and the os hamatum. It must thus be remembered that the os capitatum makes the greatest osseous contact in the carpus.
Os hamatum
The convex facet articulates with the os triquetrum, the distal surface with the basis ossic metacarpalis IV and V. Radially the os hamatum articulates with the os capitatum. The ligg. transversum et pisohamatum originate from the palmar hamulus ossis hamati.
Art. mediocarpalis: Joint capsule
The joint capsule of the distal hand joint is located at the bone-cartilage threshold of both carpal series. It forms a large number of small recesses and frequently communicates with the carpometacarpal joints.
Ligament Structures of the Hand Joint

Image: “Ligaments of wrist – anterior view.” by Henry Vandyke Carter. License: Public Domain
The meticulous hand joint, with its multitude of carpal bones, is heavily permeated with ligaments that provide stability and prevent dislocations during movement. They are localized in various layers or arranged by function, whereby each layer possesses a different number of ligaments.
Collateral ligaments
Two collateral bands are located in the regio carpalis: ligg. collaterale carpi radiale et ulnare.
Lig. collaterale carpi radiale
From the palmar corner of the proc. styloideus radii, the radial collateral ligament runs to the radial side of the os scaphoideum and the tuberculum ossis scaphoidei. It is connected to the tendon sheath of the m. flexor carpi radialis and serve to stabilize the radial side and to inhibit ulnar abduction.
Lig. collaterale carpi ulnare
The dorsal pathway starts from the proc. styloideus ulnae and the disc, and runs to the os triquetrum. The palmar pathway runs from the palmar radius to the os pisiforme. It is connate with the disc and the meniscus. It stabilizes the ulnar side and inhibits radial abduction.
Dorsal deep layer

Image: “Ligaments of wrist – posterior view.” by Henry Vandyke Carter. License: Public Domain
The ligg. intercarpalia dorsalia form the ligaments of the dorsal deep layer. They are among the intrinsic and interosseous ligaments and aid in carpal stability with their firm and strong fibre strands.
Dorsal middle layer
The middle layer of the dorsal side is formed by the lig. radiocarpale dorsale and lig. carpi arcuatum. The radiocarpal ligament runs from the radius to the os triquetrum, os lunatum and os scaphoideum, each with their own fibre pathways. This especially helps in stabilizing the art. radiocarpalis.
The proximal pathway of the lig. carpi arcuatum runs from the os scaphoideum to the os triquetrum, while the distal pathways connect the os triquetrum with the ossa trapezii. It also serves the transversal bracing of the carpal series.
Dorsal surface layer
The retinaculum extensorum forms the surface layer of the dorsal side and is a broad holding ligament for the fingers’ extensor tendons located beneath it. It forms a total of six compartments, each for one specific tendon. Intermediate septa connect the retinaculum both with the radius as well as the ulna.
Palmar deep layer
Located in the palmar deep layer are the ligg. intercarpalia palmaria. These are interosseous ligaments that connect all of the carpal bones together. They are connate with the joint capsule and thereby provide high stability against pathogenic osseous translation.
One special ligament of this group is the lig. pisohamatum, which connects the os pisiforme and os hamatum together. It closes the Loge de Guyon, an osseous ridge formed by the two bones, and protects the ramus profundus of the nervus ulnaris inside it.
Palmar middle layer
Similar to the deep layer, the middle layer also has a high number of ligamentary structures. There are the lig. carpi radiatum, lig. radiocarpale palmar and lig. ulnocarpale, whose names already hint at the respective bones that they connect and stabilize accordingly.
The lig. carpi radiatum is also known as the lig. deltoideum and connects the os capitatum with the os hamatum, os triquetrum with the os scaphoideum and os trapezoideum, and in some people the os triquetrum with the os lunatum, although this is rarely the case.
The lig. radiocarpale palmar itself has a surface and deep layer. The surface layer connects the proc. styloideus radii with the os capitatum and os triquetrum, while the deep layer connects the radius with the os scaphoideum and os lunatum. Both layers are also connate with the joint capsule and thus, provide good stability for the connected bones.
The lig. ulnocarpale runs from the proc. styloideus ulnae and disc to the os lunatum, os triquetrum, and os capitatum.
Palmar surface layer
The retinaculum flexorum and the lig. carpi palmar form the palmar surface layer.
The retinaculum flexorum is one of the deep forearm fascia and in some medical literature is also referred to as the lig. carpi transversum. It is connected to both the ulnar and radial carpal bones, and forms the primary threshold of the carpal tunnel, and also braces the arch of the hand.
The lig. carpi palmar extends between the tendons of the m. flexor carpi ulnaris and the m. palmaris longus. It is also connected with the palmar aponeurosis and envelops the tendons of the m. flexor carpi ulnaris. It thus serves to brace the aponeurosis and to protect the muscle tendons.
Functional Anatomy of the Hand Joint

Due to the structure of the proximal hand joint, the socket of the radius is not perpendicular to the longitudinal axis of the forearm, but rather forms a 20-degree angle referred to as the radial joint surface angle. Furthermore, the socket of the radius is sloped 10 degrees in the sagittal level.
This is called the sagittal radial joint angle. Both angles are essential for smooth mobility of the proximal carpal series against the surface of the radius, so as to facilitate a completely active range of motion in all possible directions of movement.
Examples of Diseases of the Hand Joint
The hand joint has a high degree of pathogenicity and the possible types of lesions are numerous, and so we will only discuss a few of the most commonly occurring diseases and symptoms.
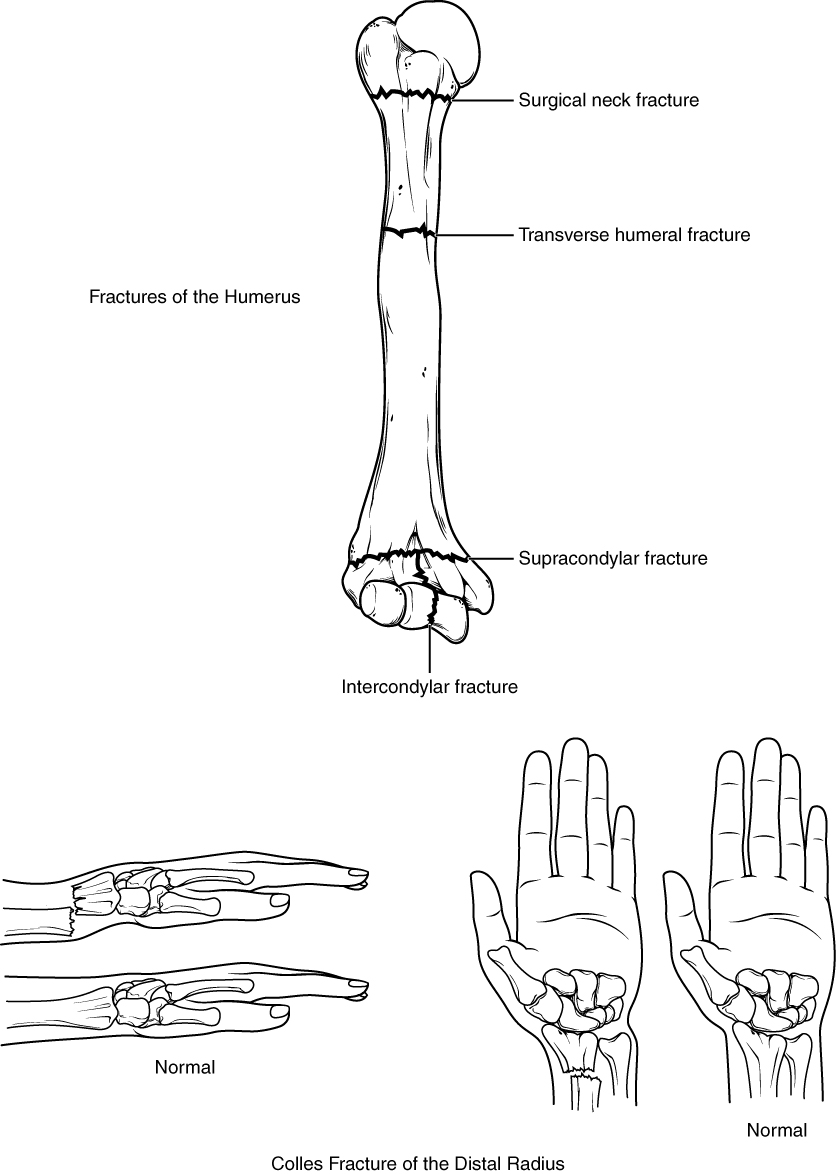
Distal radius fracture

Distal radius fracture can occur in many forms and levels of severity. Compression fracture by falling on an outstretched arm is described by the available literature as the most common type of fracture. Also described are shearing fractures, whereby ulnar, radial, dorsal and palmar fragmentation can occur with or without dislocation.
Depending on the direction of dislocation, the medial nerve can be compromised or injured, as well as the disc. Fractures without dislocation are usually treated conservatively with cast immobilization for 6 weeks, whereas fractures with dislocation are treated surgically.
Disc degeneration
In advanced age and with a patient history of heavy strain on the hand joints, painful degeneration of the interosseous disc is often diagnosed. The os lunatum and caput ulnae are non-physiologically strained, which can lead to inflammatory changes in the bone.
Furthermore, excessive strain and the resulting inappropriate care of the disc can cause ruptures. Depending on the level of injury, the disc can either be conservatively or operatively treated.
Lunatum necrosis/lunatum malacia
The causes of lunatum necrosis are not yet sufficiently understood. An overload due to excessive pressure in dorsal extension is suspected, but there are not currently any promising studies that can clearly verify this theory. Necrosis of the carpal bone leads to incongruity in the joint, and eventually to arthritis in the hand joint.
Review Questions
The answers are below the references.
1. What is the extent of the sagittal radial joint angle?
- 5 degrees
- 10 degrees
- 15 degrees
- 20 degrees
- 25 degrees
2. Which carpal bone has the greatest osseous contact in the carpus?
- Os scaphoideum
- Os pisiforme
- Os hamatum
- Os capitatum
- Os trapezium
3. How many tendon compartments make up the retinaculum extensorum of the dorsal surface layer?
- 4
- 5
- 6
- 7
- The retinaculum extensorum merely serves as a holding band for the extensor tendons and thus does not contain any tendon compartments.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comentários
Enviar um comentário