Sensory and Motor Brain Systems
Table of Contents

Image : “ear” by Paul Scott. License: CC BY-SA 2.0
The Motor System of the Brain
The motor tracts of the brain extend as efferent fibers via the spinal cord to the respective motor neurons of the skeletal muscles. The motor system comprises of the pyramidal tract (tractus pyramidalis) and the extrapyramidal system.
Structure of the Pyramidal Tract
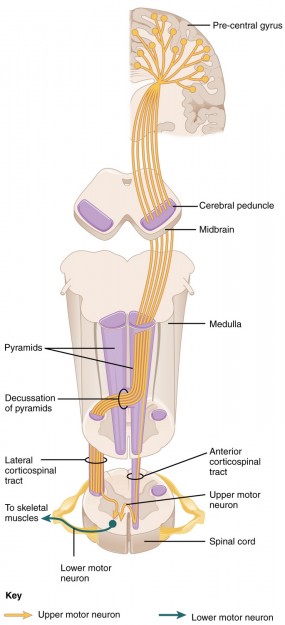
The pyramidal tract can be further subdivided into three sections: the corticospinal fibers, the bulbar corticonuclear fibers and structure of the Extrapyramidal Motor Systeme corticoreticular fibers. It controls motor functions of the body. The joint origin of these fiber tracts is located in the primary motor cortex of the telencephalon.
The primary motor cortex, or simply the motor cortex, is situated in the area of the precentral gyrus of the frontal lobe. The three sections of the pyramidal tract have the same origin but extend to different target areas according to their designation.
- The corticospinal fibers extend via the internal capsule to the spinal cord. At the level of the medulla oblongata, 80 % of the fibers cross over to the contralateral side. This fraction of fibers is called lateral corticospinal tract, subsequent to the crossing (pyramidal decussation). The remaining 20 % of fibers continue as an anterior corticospinal tract and pass over to the opposite side in their course.
Both fiber systems end in the area of the spinal cord at the interneurons, which are connected to the motor neurons of the spinal cord. This tract is responsible for transmission of impulses to cranial nerves that control muscles of face and neck.
- The bulbar corticonuclear fibers have their origin in the area of the premotor cortex, which represents the facial regions according to the motor homunculus. From this site, the fibers continue on to the motor nuclei on the contralateral side, i.e., the fibers cross over to the opposite side already on the level of the brain stem.
However, there is – in addition to the contralateral – also an ipsilateral feed to some of the nuclei, resulting in a bilateral innervation. This bilateral innervation is observable in a central facial palsy, for example. In contrast to the peripheral facial nerve paralysis, in central facial palsy, the ability of eyelid closure and the ability to raise the eyebrows are preserved because the responsible nuclei are also supplied via the contralateral side.
However, the face muscles below the area around the eyes are not bilaterally supplied, which causes, e.g., a hypokinesia of the mouth. This hypokinesia becomes especially apparent when the patient is asked to smile. In other words, the corticobulbar tract is responsible for transmitting impulses related to facial expression.
- Inside the reticular formation, the corticoreticular fibers lead to the gigantocellar reticular nucleus. They are major pathways to send impulses from muscles to brain stem of the brain for transmission of information from muscles to brain.

Structure of the Extrapyramidal Motor System
The extrapyramidal system consists of several tracts which have their origin in medulla and pons extending to the target neurons in spinal cord. It is responsible for movement, walking, and reflexes.
Part of the tracts, which are assigned to the extrapyramidal system, are the rubrospinal tract, the olivospinal tract, the vestibulospinal tract, the reticulospinal tract, and the tectospinal tract.
These tracts end collectively at the interneurons of the spinal cord, which in turn, are connected to the α- and γ-motor neurons of the spinal cord. Thereby, the extrapyramidal system has a modulating effect on the aforementioned motor neurons via the interneurons.
Symptoms of a Lesion to the Central Motor Tracts
On the one hand, the symptoms of a lesion to the central motor tracts depend on which tracts are affected by the lesion. On the other hand, the level at which the lesion occurred also plays an important role.
Depending on which tract system is affected, a distinction can be made between a spastic and flaccid paralysis. A complete, spastic paralysis (plegia) is caused when the extrapyramidal tracts are implicated, whereas an incomplete, flaccid paralysis (paresis) is generated by the involvement of only a pyramidal tract.
Because of the close anatomical and functional connection between the pyramidal tract and the extrapyramidal system, there is a spastic paresis in the majority of the centrally generated paralyzes. In contrast, a flaccid paralysis usually occurs when the second motor neuron at the level of the spinal cord is damaged.
On account of the fact that the fiber tracts cross over to the opposite side (e.g., the pyramidal tract at the level of the medulla oblongata), the respective contralateral half of the body is affected by a central impairment.
In relation to the level at which the lesion occurs, a distinction can be made between cortical lesions, lesions in the area of the internal capsule, at the level of the cerebral crus, the pons, the pyramid, the spinal cord, and at the level of the peripheral nerves.
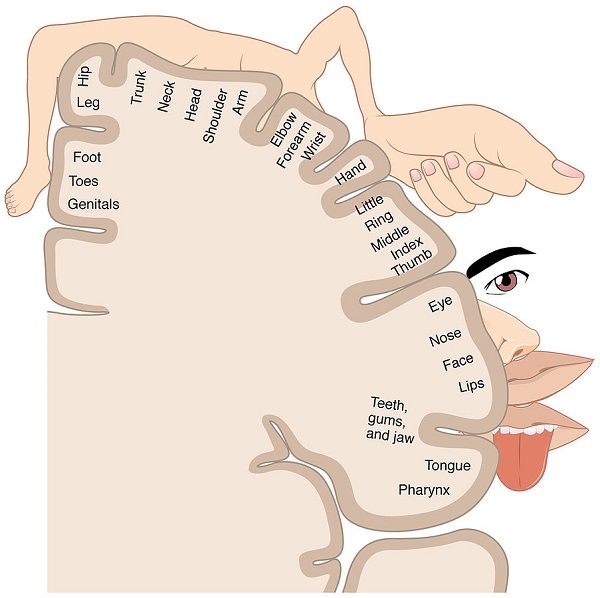
In case of an injury to the motor system in the area of the cortex, paralysis of the contralateral half of the body occurs, especially pertaining to the regions of the face and arms. This can be attributed to the fact that the arms as well as the face, constitute a relatively large proportion of the motor cortex. This amplified representation is illustrated graphically in the homunculus:
Because the pyramidal tract and the extrapyramidal system in the area of the internal capsule exhibit a common path, a lesion in this area induce contralateral spastic hemiplegia. The same clinical symptoms occur when the area of the cerebral crus is impaired.
When the area of the pons is damaged, there may be contralateral as well as bilateral pareses – depending on the extent of the lesion.
In the area of the pyramid, the fibers of the extrapyramidal system proceed further dorsally, so that an isolated lesion of the pyramidal tract may occur. In this case, the result is a flaccid paralysis (see above).
At the level of the spinal cord, the two systems, i.e., the pyramidal tract and the extrapyramidal system, are closely connected, resulting in a spastic paralysis when damaged. Because the fibers of both systems have already crossed at this point, the paresis occurs on the ipsilateral side of the lesion.
When the second motor neuron at the level of the peripheral nerves is injured, an ipsilateral flaccid paralysis ensues.
The Sensory System of the Brain
By means of the sensory system, different sensations from the periphery are perceived by receptors and subsequently conveyed to the brain. The different qualities of sensory perceptions are in partly assembled in distinct systems or tracts, respectively.
The conveyed qualities include, for instance, pain, temperature and the crude sense of touch; these three qualities are summarized by the term protopathic sensibility. Another system is represented by epicritic sensibility, which comprises the fine sense of touch in the area of the face.
Another quality, which is conveyed via the sensory system, is proprioception. By means of proprioception, a spatial perception of the body’s own extremities is maintained.
Additionally, this system receives further information from the muscle and tendon spindles, in order to obtain information about the position of the joints as well as the velocity and direction of movement. Furthermore, the muscular power, which is generated upon movement of the joint, is being perceived and transferred to the proprioceptive system. Taken together, these three kinds of information are designated as follows:
- Joint position sense
- Kinaesthetic sense
- Strength sense
Within the proprioceptive system, a distinction can be made between unconscious and conscious proprioception. Both systems are relayed to different target areas.
The information gathered by unconscious proprioception arrives at the cerebellum via the spinocerebellar tract. In comparison, information obtained by conscious proprioception reaches the thalamus via the dorsal column system and a switch in its nuclei, where it is transferred to the somatosensory cortex and thus enters consciousness (see below).
Among the receptors of the somatosensory system are, for example, the skin and joint receptors. The receptors always constitute the first neuron of the respective sensory tract.
The above-mentioned qualities are conducted in the sensory system through three tracts, some of which can be further subdivided. Among these tracts are the anterolateral system, the dorsal column system as well as the spinocerebellar tracts.
Tracts and Connections of the Anterolateral System
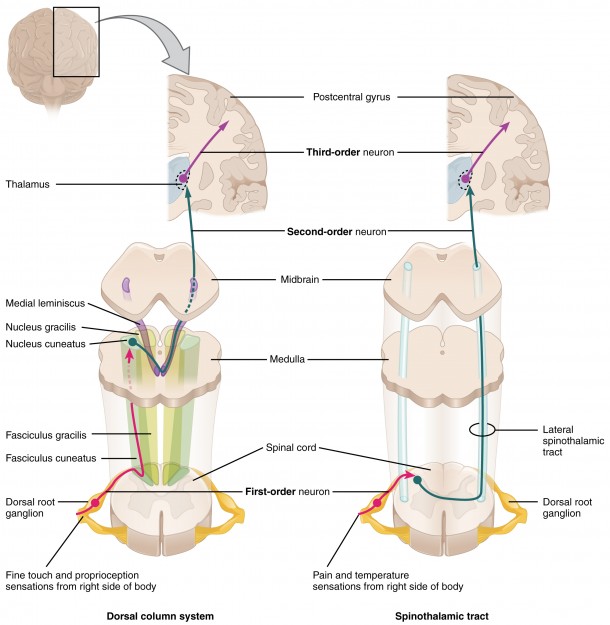
The anterolateral system can be further divided into the anterior spinothalamic tract and the lateral spinothalamic tract. The anterior spinothalamic tract conveys the crude sense of touch, while the lateral spinothalamic tract serves to conduct the information related to the sense of pain and temperature.
The perikarya of the second neurons of the anterior spinothalamic tract are located in the posterior horn, and the perikarya of the second neurons of the lateral spinothalamic tract are found in the gelatinous substance of the spinal cord.
In contrast to the lateral spinothalamic tract, the second neuron of the anterior spinothalamic tract may be 15 segments above or up to two segments below the first neuron. The axons of both tracts pass over to the opposite side on the level of the spinal cord in the area of the anterior commissure.
The ensuing path of both tracts is identical, too. In the area of the ventral posterolateral nucleus of the thalamus, the connection to the third neuron is established, whose axon extends to the postcentral gyrus.
Tracts and Connections of the Dorsal Column System
The dorsal column system is composed of the gracile fasciculus and the cuneate fasciculus. Both of them convey information of the fine sense of touch, including sensitivity to vibrations (transferred via the lamellar corpuscles of the skin) as well as conscious proprioception.
In conjunction with the conscious proprioception, the information from the lower extremity is conveyed through the gracile fasciculus, while the information from the upper extremity is conveyed through the cuneate fasciculus.
The axons of the first neurons extend inside of the medulla oblongata to the homonymous nuclei, i.e., the axons of the gracile fasciculus span to the gracile nucleus, and the axons of the cuneate fasciculus stretch to the cuneate nucleus. The respective nucleus constitutes the second neuron of the dorsal column system.
The axons of the second neurons cross over to the opposite side in the brain stem area and subsequently extend inside the medial lemniscus to the ventral posterolateral nucleus of the thalamus. At this point, the connection to the third neuron is established, and the information is transferred to the postcentral gyrus.
Paths and Connections of the Spinocerebellar Tracts
The quality of unconscious proprioception is relayed within the spinocerebellar tracts; this is realized via the anterior and posterior spinocerebellar tracts.
The anterior spinocerebellar tract passes proportionately to the contralateral side at the level of the spinal cord, while in the posterior spinocerebellar tract, the information passes to the cerebellum exclusively in an ipsilateral manner.
The second neuron of the anterior spinocerebellar tract is situated in the central part of the grey matter of the spinal cord, while the second neuron of the posterior spinocerebellar tractis located in the thoracic nucleus. The thoracic nucleus can be found in the area of the posterior horn of the grey matter.
Subsequently, the axons extend to the cerebellum, while the fraction of the anterior spinocerebellar tract, which had previously crossed over, passes to the ipsilateral side again, before entering the cerebellum. Thereby, the cerebellum exclusively receives ipsilateral information from the spinal cord via the spinocerebellar tracts.
The information is conveyed through a different respective peduncle to the cerebellum. The axons of the anterior spinocerebellar tract continue via the superior cerebellar peduncle, and the axons of the posterior spinocerebellar tract extend via the inferior cerebellar peduncle to the cerebellar vermis.
Pathology of a Lesion to the Sensory System
The pathology of a lesion to the sensory system is comparable to a motor system impairment insofar as it depends on the affected fiber tract and its path.
The result of cortical or subcortical lesions are paraesthesiae, which often manifest themselves as sensations of tingling and numbness in the contralateral half of the body, which are frequently distally emphasized.
In case of an injury to the thalamus or a subthalamic lesion, respectively, the information from the sensory system does not enter consciousness anymore, causing the cessation of the sensory perception on the contralateral half of the body.
In the event of damage to one of the three sensory tracts, different symptoms develop according to the path of the tract and its transferred qualities; the unconscious information conveyed through the spinocerebellar tracts, however, is an exception, which induces sensorimotor deficits.
Deficiency of the anterolateral system
In case of a complete lesion to the anterolateral system, there is a loss of the crude sense of touch (anterior spinothalamic tract) as well as a loss of the sensation of pain and temperature (lateral spinothalamic tract). This deficit occurs on the contralateral side because of both fiber tracts of the anterolateral system cross over to the opposite side at the level of the spine.
In addition to a complete lesion, there may be an isolated deficit of a fiber tract, so that only the correspondingly transferred quality on the contralateral side is canceled.
Deficiency of the dorsal column system
When the dorsal columns are lesioned, the proprioception, as well as the fine sense of touch on the ipsilateral side, is affected. The ipsilateral pathology is explained by the fact that the fibers of the dorsal column do not cross over to the opposite side before the level of the brain stem is reached.
Possible causes for an impairment are, for instance, a vitamin B12 deficiency, which can occur in the context of alcoholism. This clinical picture is called subacute combined degeneration of the spinal cord (SACD), in which the lateral columns are affected, in addition to the dorsal columns.
Review Questions
The correct answers can be found below the reference list.
1. Which statement about the pyramidal tract is not true?
- The pyramidal tract is composed of the corticospinal fibers, the bulbar corticonuclear fibers, and the corticoreticular fibers.
- The pyramidal tract is attributed to the motor system.
- In their course, 100 % of the fibers cross over to the opposite side.
- Some of the motor nuclei receive a double innervation.
- In case of a lesion of the pyramidal tract, the motor deficits occur ipsilaterally.
2. Which statement about the sensory system is not true?
- Within the sensory system, a distinction can be made between the anterolateral system, the dorsal column system and the spinocerebellar tracts.
- The term protopathic sensibility comprises the sense of pain, temperature and crude touch.
- Epicritic sensibility conveys the fine sense of touch in the area of the face.
- The quality of unconscious proprioception is relayed via the thalamus to the somatosensory cortex.
- The fibers of the spinocerebellar tracts transfer information exclusively from the ipsilateral spinal cord to the cerebellum.
3. Which statement about lesions of the sensory system is true?
- A lesion to the area of the thalamus results in the complete cessation of the conscious sensory perception on the ipsilateral half of the body.
- When the spinothalamic tract is deficient, a loss of the sensation of pain and temperature is induced.
- Damage to the anterolateral system inflicts sensory deficits on the ipsilateral half of the body.
- In the event of a deficit of the dorsal column system, a loss of the perception of the crude sense of touch is induced.
- When the dorsal column is injured at the level of the spinal cord, the sensory deficits occur on the ipsilateral half of the body.



Comentários
Enviar um comentário