Structure, Functions, and Diseases of the Autonomic Nervous System (ANS)
Table of Contents
Functional Organisation of the Vegetative/Autonomic Nervous System
The vegetative or autonomic nervous system (from Greek: autos = self; nomos = law) uses both sensory and efferent neurons, which especially control the function of the internal organs.
The characteristic feature of the autonomic system is that its efferent nerves emerge as medullated fibres from the brain and spinal cord, are interrupted in their course by a synapse in a peripheral ganglion and are then relayed for distribution as fine non-medullated fibres. In this respect they differ from the cerebrospinal efferent nerves, which pass without interruption to their terminations.
The autonomic nervous system allows the higher brain centers (cerebral cortex and limbic system) to subconsciously control organs of the autonomic nervous system. It controls functions such as sexual arousal, urination, digestion and cardiorespiratory functions.

Image: “Diagram showing the divisions of the nervous system.” by Fuzzform. License: CC BY-SA 3.0
Autonomic nervous system divisions
The autonomic nervous system also has two divisions: the sympathetic division and the parasympathetic division on anatomical, functional, and to a considerable extent, pharmacological grounds. The two divisions have antagonistic effects on the internal organs they innervate.
Anatomically, the sympathetic nervous system has its motor cell stations in the lateral grey column of the thoracic and upper two lumbar segments of the spinal cord. The parasympathetic system is less neatly defined anatomically since it is divided into a cranial outflow, which passes along the cranial nerves III, VII, IX and X, and a sacral outflow, with cell stations in the 2nd, 3rd and sometimes 4th sacral segments of the cord.
Sensory neurons
The main input of the ANS particularly comes from autonomic sensory (viscerosensory) neurons, which are usually associated with interoceptors and act as sensory receptors in blood vessels, visceral organs and muscles. These neurons, which have the task to transduce information to the CNS, are usually located in the stomach and the lung.
Unlike the signals that are triggered by a nice-smelling odour or a delicious looking meal, the inner sensory signals are normally not experienced consciously, although the activation of interoceptors can indeed advance into consciousness. Here, two typical examples would be the pain caused by damaged intestines or an angina pectoris (chest pain) caused by inadequate perfusion of the myocardium.
“Somatic (afferent) sensory neuron cell body – only 1 neuron is involved” Image created by Lecturio
Efferent neurons
On the other hand, efferent neurons forward the nerve impulses from the CNS to the target tissue (smooth muscle, heart muscle or glands) and regulate visceral activities by an increase (excitation) or decrease (inhibiting).
Nerves of the sympathetic and parasympathetic nervous system are responsible for these oppositional effects.
Sympathetic neurons accelerate i.e. the heartbeat and support the processes or effort of the body, and enable a ‘fight-or-flight’-reaction. This allows an improvement in performance and consequently, is stimulated in states of excitement, activity and stress.
Parasympathetic neurons in contrast decelerate the heartbeat and induce a ‘rest-and-digest’-reaction. These neurons are responsible for relaxation, recreation and inducing the regeneration of vital energy reserves.
Efferent responses are not controlled consciously, thus the activity of the autonomic nervous system (ANS) is unintentionally. So-called ‘lie detector-tests’ are based on several autonomous reactions, since the pulse cannot be manipulated intentionally to half of the standard value. However, some people can alter their autonomic activities by applying adequate relaxing techniques.
Structure of the ANS/VNS
The first of the two motor neurons in every motoric signalling pathway is called a preganglionic neuron. Its soma is located in the brain or spinal cord and its axon, on the other hand, leaves the CNS as a part of a cranial nerve or spinal nerve.
Generally, the preganglionic neuron connects with an autonomic ganglion, where it forms a synapse with the second neuron of the signalling pathway, the postganglionic neuron. Soma and dendrites of the postganglionic neuron are located in an autonomic ganglion, where they form synapses with one or more preganglionic neurons.
The autonomic nervous system transduces nerve impulses from preganglionic neurons to autonomic neurons, where the signals are forwarded to postganglionic neurons and then transmitted to the target tissue.
The following example is to be said:
Spinal cord (CNS) → preganglionic neuron → autonomic ganglion → postganglionic neuron → heart (target tissue/effector)
Preganglionic neurons
Thoracolumbar part
The sympathetic part of the ANS is also called a thoracolumbar part since the somas of the preganglionic neuros are located in the lateral horn of the twelve thoracic segments, as well as the first two or three lumbar segments of the spinal cord.
Craniosacral part
On the other hand, the parasympathetic part of the ANS is also referred to as a craniosacral part because the somas of the parasympathetic preganglionic neurons are located in the nuclei of four cranial nerves in the area of the brain stem, as well as in the lateral horns of the second to fourth sacral segment of the spinal cord.
Autonomic ganglia
Autonomic ganglia are divided into three groups:
- Sympathetic chain ganglia
- Sympathetic prevertebral ganglia
- Parasympathetic ganglia
Sympathetic ganglia are located where the synapses between preganglionic and postganglionic sympathetic neurons interact.
Sympathetic chain ganglia
Ganglia of the sympathetic trunk (paravertebral ganglia) are arranged in a vertical column on each side of the spine and reach from the base of the skull down to the coccygeal bone. For the most part, organs above the diaphragm are innervated by postganglionic axons of the ganglia of the sympathetic trunk.
Sympathetic prevertebral ganglia
Sympathetic prevertebral ganglia are located on the ventral side of the spine close to the large abdominal arteries. On the contrary, postganglionic axons of paravertebral ganglia innervate organs inferior to the diaphragm. The 3 largest prevertebral ganglia are:
- Coeliac ganglion (located right underneath the diaphragm)
- Superior mesenteric ganglion (located in the epigastric region)
- Inferior mesenteric ganglion (located in the umbilical region)
The branches of the sympathetic ganglionic chain have somatic and visceral distribution.
Somatic distribution
Each spinal nerve receives one or more grey rami from a sympathetic ganglion which distributes postganglionic non medullated sympathetic fibres to the segmental skin area supplied by the spinal nerve. These fibres are vasoconstrictor to the skin arterioles, pseudo motor to sweat glands and pilomotor to the cutaneous hairs.
Visceral distribution
Postganglionic fibres to the head and neck and to the thoracic viscera arise from the ganglion cells of the sympathetic chain. Those to the head ascend along the internal carotid and vertebral arteries, whereas those to the thoracic organs are distributed by the cardiac, pulmonary, and oesophageal plexuses.
The abdominal and pelvic viscera, however, are supplied by postganglionic fibres which have their cell stations in more peripherally placed prevertebral ganglia—the coeliac, hypogastric, and pelvic plexuses—whichreceive their preganglionic fibres from the splanchnic nerves
Parasympathetic Ganglia

Preganglionic axons of the parasympathetic nervous system form synapses with postganglionic neurons in terminal or intramural ganglia. For the most part, the ganglia are located near to or inside the wall of an organ.
Axons of preganglionic parasympathetic neuronsare usually longer than most of the axons of preganglionic sympathetic neurons since they reach from the CNS all the way to an intramural ganglion of the innervated organ.
Afferent parasympathetic fibres
Visceral afferent fibres from the heart, lung and the alimentary tract are conveyed in the vagus nerve. Sacral afferents are conveyed in the pelvic splanchnic nerves and are responsible for visceral pain experienced in the bladder, prostate, rectum, and uterus.
Although afferent fibres are conveyed in both sympathetic and parasympathetic nerves, they are completely independent of the autonomic system. They do not relay in the autonomic ganglia and have their cell stations, just like somatic sensory fibres, in the dorsal ganglia of the spinal and cranial nerves. They simply use the autonomic nerves as a convenient anatomical conveyor system from the periphery to the brain.
Postganglionic neurons
Axons of preganglionic sympathetic neurons can be connected to postganglionic neurons by the following three possibilities after they have headed to the ganglia of the sympathetic trunk:
- An axon can form a synapse with a postganglionic neuron directly in the first reached ganglion.
- An axon can ascend or descend to a higher or lower located ganglion before it is wired up with the postganglionic neuron, which runs vertically next to the sympathetic trunk.
- An axon can run through the sympathetic ganglion without forming a synapse and end in a prevertebral ganglion to be switched over to the postganglionic neuron.

A single preganglionic sympathetic fiber has many branches, which is the reason why it can be connected with more than 20 or more postganglionic neurons over synapses. The postganglionic axons typically end in different target tissues.
In these ganglia, presynaptic neurons only transmit to four to five postsynaptic neurons. They all individually provide a visceral target tissue and, as a consequence, this target tissue can be controlled separately by parasympathetic fibers.

Autonomic plexuses
Axons, sympathetic and parasympathetic neurons form networks that are called autonomic plexuses. They run along large arteries and can be found in thorax, abdomen and pelvis. The large cardiac plexus in the thorax is in charge of the innervation of the heart and the pulmonary plexus for the bronchial tree.
The largest autonomic plexus is the coeliac (solar) plexus, which passes on to the liver, gall bladder, stomach, pancreas, spleen, kidneys, adrenal cortex, testicles and ovaries.
Neurotransmitter and Receptors of the ANS/VNS
Neurotransmitters are assigned to receptors – integral membrane proteins that are located in the plasma membrane of the postsynaptic neuron or a cell of the target tissue.
We differentiate between cholinergic and adrenergic neurons.
Cholinergic neurons and receptors
The ANS includes the following cholinergic neurons:
- All sympathetic and parasympathetic preganglionic neurons
- Sympathetic postganglionic neurons for most of the sweat glands
- All postganglionic parasympathetic neurons
Cholinergic neurons release the neurotransmitter acetylcholine (ACh) which is stored in synaptic vesicles and liberated by exocytosis. After that, it diffuses through the synaptic cleft and binds to specific cholinergic receptors.
Cholinergic receptors are further subdivided into nicotinergic and muscarinergic receptors that both bind ACh.
Nicotinergic receptors are embedded in sympathetic and parasympathetic postganglionic neurons, as well as in the neuromuscular junction. They bear this term because nicotine simulates the action of ACh after binding to the receptors. In non-smokers, this substance is not traceable since nicotine is not a physiologically present substance in the human organism.
However, in the plasma membrane of all target tissues (smooth muscle, myocardium and glands), the muscarinergic receptors are present, which are supplied by parasympathetic postganglionic axons. In several receptors, occurs an inhibition, whereas, in others, an excitation. Similarly, sweat glands have muscarinergic receptors which results in increased sweating.
Acetylcholine is quickly deactivated by the enzyme acetylcholine esterase and thus the effects triggered by cholinergic neurons are short.
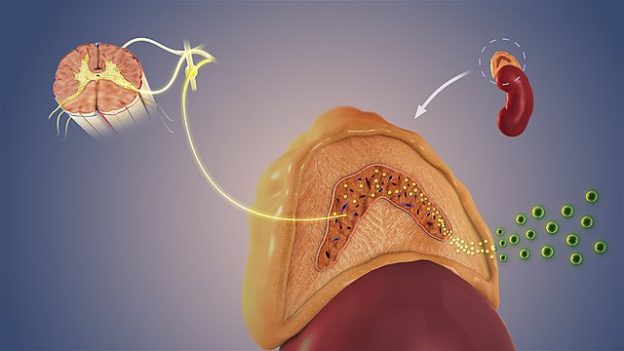
Adrenergic neurons and receptors
Noradrenaline (NAdr) is released in the ANS by adrenergic neurons. A great number of postganglionic sympathetic neurons are adrenergic. The NAdr is stored, just like ACh, in synaptic vesicles, released by exocytosis, which diffuses through the synaptic cleft and binds to specific adrenergic receptors of the postsynaptic membrane. The consequence is an excitation or an inhibition of the effector cell.
Noradrenaline, as well as adrenaline, bind to adrenergic receptors. The NAdr can be released as a neurotransmitter by sympathetic postganglionic neurons or as a hormone by the adrenal medulla, into the blood. Adrenaline is solely released as a hormone.
Also, the adrenergic receptors can again be subdivided into two subtypes which are innervated by most of the postganglionic sympathetic neurons. They are called alpha (α)-receptors and beta (β)-receptors, which are further subdivided according to their specific answers and the corresponding binding properties (α1, α2, β1, β2, etc.).
Broadly speaking, an activation of the α1- and β1-receptors induces an excitation, whereas α2- and β2-receptors yield an inhibition of the target tissue.
Autonomic reflexes
Answers that are triggered by nerve impulses in an autonomic reflex arc are called autonomic reflexes. The play a key role in the following processes:
- Blood pressure (i.e. by adjusting the heart rate)
- Digestion (adjustment of motility and muscle tone in the GI tract)
- Defecation
- Urination (regulating the opening and closing of the sphincter)
The main control and integration center of the ANS is the hypothalamus, which receives sensory information about visceral functions (smell, taste and temperature etc.). Signals of the limbic system, which cohere with emotions, influence this process as well. The signals coming from the hypothalamus affect autonomous centres in the brain stem (truncus cerebri), as well as in the spinal cord (medulla spinalis).
An autonomic reflex arc consists of the following components:
Receptor
- The distal end of a sensory neuron is the receptor of an autonomic reflex arc, which reacts to a Stimulus and triggers a nerve impulse. Usually, autonomic sensory receptors are associated with interoceptors.
Sensory neurons
- The sensory neuron forwards nerve impulses to the CNS.
Integration centre
- The main integration centres for autonomic reflexes are located in the hypothalamus and the brain stem. Some autonomic reflexes are situated in the integration centres of the spinal cord, which are mostly responsible for urination and defecation.
- Connectivity: interneurons of the CNS forward signals from the sensory neurons to motor neurons.
Motor neurons
- Signals triggered by integration centres leave the CNS, via motor neurons, towards the target tissue. Two motor neurons connect the CNS in an autonomic reflex arc with the effector. The impulse is transduced by the preganglionic neuron to an autonomic ganglion from where it is forwarded through the postganglionic neuron to the target tissue.
Target tissue (effector)
- The effectors of the autonomic reflex are the smooth muscles, the heart muscle or the glands.
Diseases of the ANS/VNS
In contrast to the somatic nervous system, the tissues that are innervated by the ANS also keep running while damaged. The heart, for example, keeps beating if it is isolated from its vegetative nerve fibers. Smooth muscle cells of the gastrointestinal tract contract independently and rhythmically, and glands produce several substances without being controlled via the ANS. For this reason, most autonomous responses cannot be deliberately changed or suppressed by a significant rate.
Contrary to the somatic nerve system, the tissues which are innervated by the ANS also work after a damage of the neural nourishment. The heart, for example, keeps beating if it is disrupted from its vegetative nerve fibers. Smooth muscle cells of the GI tract contract independently and rhythmically and also glands produce several substances without the control of the ANS. This is why most autonomic answers cannot be changed or suppressed intentionally to a greater extent.
However, the autonomic/vegetative nervous system can, as well, be affected by a pathological impairment
Horner‘s Syndrome
Horner’s Syndrome describes the damaged sympathetic nerves of one side of the face, which affects the sympathetic output of the superior cervical ganglion. This can be caused by an injury, a disease or a hereditary mutation. A commonly examined scenario is where Horner´s syndrome can present in a Pancoast lung tumor – its metastatic spread can invade the sympathetic chain and cause this syndrome.
Horner’s Syndrome is characterized by the following symptoms:
- Ptosis (dropping of the upper eyelid)
- Miosis (constricted pupil)
- Enophthalmos (posterior displacement of the eyeball)
Further diseases of the autonomic nervous system
- Raynaud’s phenomenon
- Autonomic dysreflexia
- Autonomic neuropathy
- Dysautonomia
- Hyperhidrosis
- Megacolon
- Sudeck’s disease
- Vagotomy
Autonomic nervous system dysfunction
Autonomic nervous system dysfunction (also known as dysautonomia) leads to non- functional organs of the autonomic nervous system. Some of the causes of this dysfunction include autonomic neuropathy, HIV/AIDS, multiple sclerosis, paraneoplastic syndromes and Parkinson’s disease. Patients present with features of unopposed efferent neuronal function which include anihydrosis, anxiety, constipation, orthostatic hypotension, tachycardia, vertigo, and bowel incontinence, difficulty in swallowing exercise intolerance and chronic fatigue.
Treatment of autonomic nervous system dysfunction entails symptomatic relief using a wide array of drugs such as PPIs. H2 receptor antagonist can be used to reverse hyperacidity and reflux while anticholinergic agents such as scopolamine reverse effects such as hyperhidrosis and tachycardia.



{kind=link}
Comentários
Enviar um comentário