Cardiovascular Response to Exercise
Table of Contents

Image: “Running woman.” by Peter van der Sluijs – Own work. License: CC BY-SA 3.0
Isotonic and Isometric Resistance Exercise
Isotonic resistance exercises involve the shortening and lengthening of the muscle. Isotonic resistance exercise, also known as dynamic constant external resistance (DCER) builds
both muscle strength as well as endurance. Examples include any
exercise that involves lifting and lowering weights, lunges, or opening
and closing joints, such as pressing and curls or squatting, are
considered isotonic.
Similar changes in HR, SVR, and muscle blood flow is seen in isometric exercise, except:
- Blood flow rises after each contraction
- Results in an active hyperemia blood flow pattern
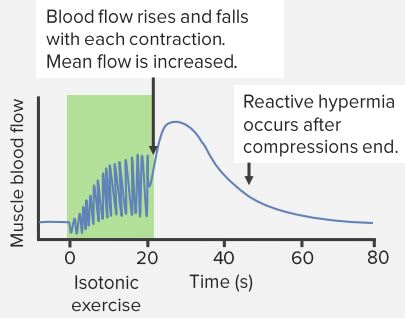
“Isotonic Resistance Exercise” Image created by Lecturio
Isometric exercises, on the other hand, challenge your muscles
without any joint movement and the length of the muscle remains
consistent. The resistance is due to the force of gravity. It is often referred to as ‘static strength training’ as the person only holds a certain position rather than moving.
An example would be performing a plank, where your core muscles are
strengthened while at a fixed length or carrying heavyweights such as
shopping bags where your arm muscles are contracted although they are
not necessarily moving.
Blood Pressure Effects of the Valsalva Maneuver
The Valsalva maneuver describes a forceful exhalation against a closed epiglottis, which happens whenever you strain to lift something heavy and especially in isometric exercise.
The Valsalva maneuver increases intra-abdominal pressure, which is
necessary to stabilize your spine from within but also causes a dramatic
rise in blood pressure. The Valsalva maneuver can cause blood pressure to rise from a normal resting level of 120 mmHg to over 300.
The blood pressure changes occurring as a result of this maneuver are:
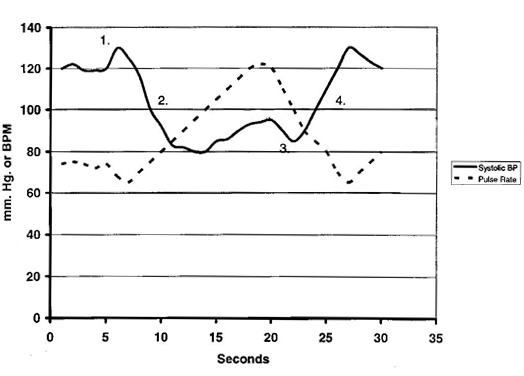
Image:
“Systolic blood pressure and pulse rate changes during Valsalva
maneuver.” by T.torda at English Wikipedia – Own work. License: Public Domain
On the application of full expiratory force, the blood from the pulmonary circulation shifts into the left atrium. This increases the stroke volume and an initial rise in systolic blood pressure, at 5 seconds, labeled as 1 in the graph.
Due to increased intrathoracic pressure, the venous return
decreases. This results in a decrease in the stroke volume. The blood
pressure initially drops to 5—15 seconds (labeled as 2) but soon vasoconstriction occurs, which causes a slight rise in the blood pressure. The decrease in the stroke volume causes reflex tachycardia shown in the graph.
As the pressure of the chest cavity decreases after exhalation, the pulmonary vessels fill with blood again. This causes decreased return of blood to the left atrium
causing a decrease in blood pressure at 20—23 seconds (labeled as 3).
The decrease in the stroke volume is soon compensated by an increase in
the venous return. The blood pressure begins to rise again from 23—27
seconds.
The stroke volume initially rises above normal (labeled 4) due to a rush of blood into the ventricle and returns to the normal value at 30 seconds. The pulse rate, which was increased due to decreased cardiac output also returns to the normal value.
“ABP Response to Resistance Exercise” Image created by Lecturio
Endurance Training
When a person engages in daily or regular exercise, certain responses
are produced in their body to increase its efficiency and capacity.
The cardiac output increases as the rate of oxygen
demand increases. However, this linear relationship has a certain limit
after which the cardiac output stays constant. The heart rate increases as the oxygen demand increases in order to maintain a constant cardiac output.
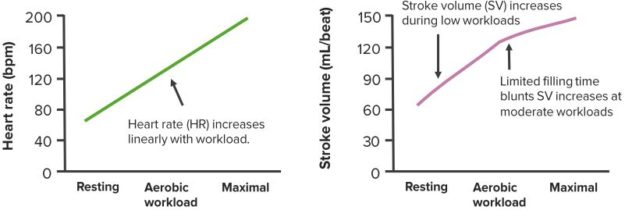
“CO Changes in Endurance Exercise” Image created by Lecturio
When a person is at rest, only 20 % of the cardiac output goes to the skin and the skeletal muscles.
However, when they are exercising, more blood needs to flow toward the
highly metabolic skeletal muscles. This is to allow the provision of
more oxygen and removal of waste products such as carbon dioxide. It is
estimated that up to 80 % of the cardiac output is supplied to the
skeletal muscles and the skin in exercise.
If the external temperature is higher, then more blood flows to the skin in order to keep the internal body temperature constant.
The long-term cardiovascular changes occurring as a result of endurance training include little change in the cardiac output at rest and sub-maximal exercises.
However, at the maximal level of exercise, the cardiac output
increases by up to 30 %. After training, stroke volume is increased at
rest, during sub-maximal and at maximal training. The heart rate, on the other hand, is decreased at rest and sub-maximal training. It may remain unchanged during maximal training.
The increase in stroke volume in endurance training is due to an increase in the blood volume. This is due to increases in the venous return, thus to an increase in end-diastolic volume. In addition, hypertrophy of the cardiac muscles also occurs, which increases the overall force of contraction.
Endurance training also increases the number of capillaries in the skeletal muscles. Therefore, more blood can flow. As the capacitance of the blood increases because of new capillaries formed, the total peripheral resistance decreases. As
a result, plasma volume increases within two to three weeks of
endurance training and more blood reaches the right atrium. The left
ventricle then can pump more blood into the aorta.
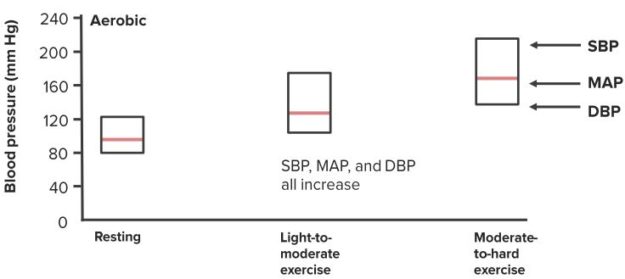
Blood Pressure Response to Endurance Training
Because of the formation of new capillaries, the arterial blood pressure decreases as a result of endurance training in normotensive persons.
After training, the blood pressure at rest, during sub-maximal exercise
and maximal exercise is lower than before. This decrease is greater in hypertensive patients. For instance, if the decrease in normotensive person is 3 mmHg, the decrease in hypertensive patients is 10 mmHg.
Skeletal Muscle Effects of Chronic Endurance Training
Long-term exercise results in hypertrophy of a
specific group of muscles. Sometimes, for counterbalance, the opposite
group of muscles also undergoes an increase in muscle mass, a phenomenon
known as cross education.
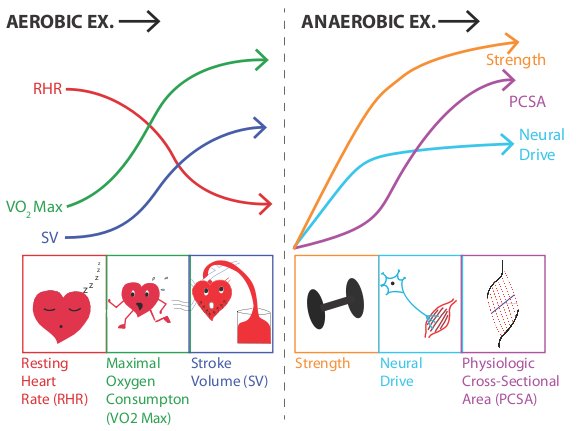
Image: “Summary of adaptations to long-term aerobic and anaerobic exercise.” by Plin7 at English Wikipedia. License: CC BY-SA 3.0
The metabolic capacity of the muscles also changes
with endurance exercise. Muscles performing the anaerobic exercise
(white fibers) will start producing more glycolytic enzymes. Similarly, muscles performing aerobic exercise (red fibers) will develop more blood capillaries and mitochondria.
Additionally, oxygen extraction from the blood increases, resulting in the prompt supply of energy.
The type of muscle fibers remains unchanged and the presence of certain type of muscle fibers in certain athletes is genetic.
Aerobic exercise training results in an increase in oxygen consumption and stroke volume while the resting heart rate decreases. Similarly, the anaerobic exercise training
results in an increase in muscle strength, neural drive, and
physiologic cross-sectional area. After anaerobic training such as
sprinting and weightlifting the heart rate stays elevated for several
hours.



{kind=link}
{kind=link}
{kind=link}
Comentários
Enviar um comentário