Medical Psychology and Sociology: Foundations of Biopsychology
Biopsychology (behavioral neuroscience) is concerned with the mutual influence of the body’s biological processes and our behavior and experience. This article discusses the states of stress, activation, consciousness and sleep, including both background issues and pathologies. Learn how to interpret a wake and sleep EEG, which stress models are important for exams and what happens during the fight or flight response. With the right preparation, the ‘preliminary examination’ that causes you such mental stress will only cause eustress.
Table of Contents
- The connection between stress and disease
- Three Main Types of Stressors
- Stress models
- Our behavior and the brain: the electroencephalogram (EEG)
- Evoked potentials/event-related potentials
- States of activation and consciousness
- The orienting response and the defensive reaction
- Sleep: 30% of our lifetime
- Stages of sleep
- Sleep disturbances/Insomnia
- Review Questions
- References
Are you more of a visual learner? Check out our online video lectures and start your psychology and sociology course now for free!

The connection between stress and disease
When our coping mechanisms are exceeded, our body responds with an adaptation response: stress. The aim is then to restore the balance (homeostasis) between the person and their environment.
Note: Stress is a response, not a stimulus. Stressors originate in the environment or from within the person him/herself:
- Mental Stressors: isolation, time pressure, critical life events (birth, marriage, loss of someone beloved, etc.)
- Physiological Stressors: disease, noise, cold, lack of sleep
Three Main Types of Stressors
| Types of Stress | Description |
| Catastrophes | Unpredictable, large-scale events like natural disasters or terrorist attacks Easily identified as very stressful |
| Significant life changes | Include events such as moving, marriage, divorce, death of a loved one Most impactful during young adulthood |
| Daily hassles | Everyday irritations in life Can accumulate to cause health issues |
Effects of stress on psychological functions
Low to moderate amounts of stress can improve psychological functioning. It provides more energy and motivation for cognitive activities. If stress is sub-optimal, the psychological function can be compromised. It can lead to fatigue, irritability and the inability to concentrate.If stress is sub-optimal, the psychological function can be compromised. It can lead to fatigue, irritability and the inability to concentrate.
If stress is accompanied by a lack of control, over time, this can lead to learned helplessness. Learned helplessness is a sense of exhaustion and lack of belief in one’s ability to manage situations.
Emotional stress outcomes/response to stressors
Physiological stress-activated two parallel systems:- Sympathetic nervous system and
- Hypothalamic-pituitary-adrenal axis (HPA axis)
The fight or flight response, responds to acute stressors (fast-acting).
The stress hormones Adrenaline and Noradrenaline are secreted from the medulla zone of the Adrenal gland.
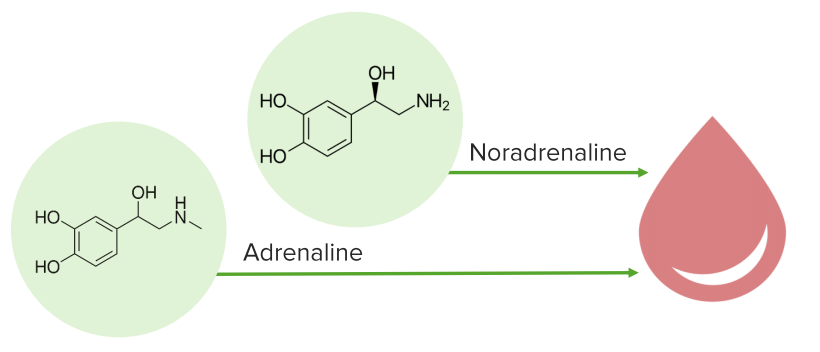 ⇒ Increased heart rate, respiratory rate, blood flow to skeletal muscles, slows digestion, dulls pain
⇒ Increased heart rate, respiratory rate, blood flow to skeletal muscles, slows digestion, dulls pain2. Hypothalamic-pituitary-adrenal axis
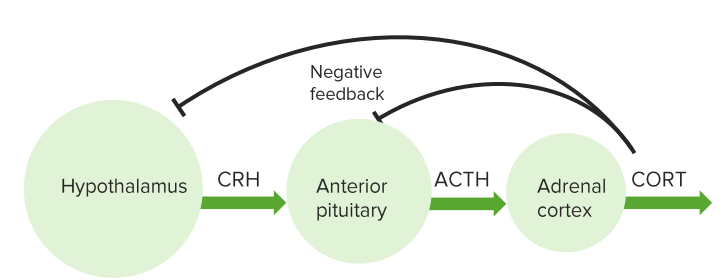 Hypothalamus releases corticotropin-releasing hormone (CRH). CRH stimulates the pituitary gland to release adrenocorticotropic hormone (ACTH). ACTH then signals the adrenal glands to release cortisol into the blood stream.
Hypothalamus releases corticotropin-releasing hormone (CRH). CRH stimulates the pituitary gland to release adrenocorticotropic hormone (ACTH). ACTH then signals the adrenal glands to release cortisol into the blood stream.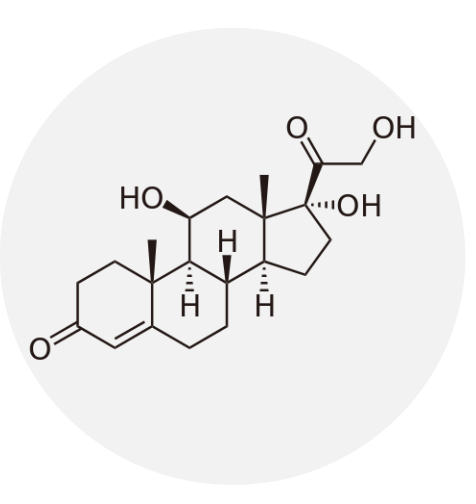 Cortisol is a glucocorticoid, a hormone that shifts the body from sugar to fat as an energy source. It keeps blood-sugar levels high during stressful situations, providing the brain with an ample supply. Prolonged release of cortisol due to chronic stress can have harmful effects:
Cortisol is a glucocorticoid, a hormone that shifts the body from sugar to fat as an energy source. It keeps blood-sugar levels high during stressful situations, providing the brain with an ample supply. Prolonged release of cortisol due to chronic stress can have harmful effects:- Inhibits activity of white blood cells and immune system
- Increases vulnerability to illness
Emotional stress
Emotional stress is correlated with worse health outcomes, and may exacerbate-existing underlying conditions (i.e. cardiac, anxiety) and may contribute to the development of mood disorders.Individuals may respond differently to the same stressor depending on appraisal and circumstance. We either confront or avoid (avoidance) stressors. Avoidance can be accompanied by habits such as substance abuse and unhealthy eating.
In response to high stress, some develop post-traumatic stress disorder (PTSD). PTSD is characterized by the symptoms of:
- Avoidance
- Hyperarousal
- Re-experiencing
Managing stress
There is an optimal range of stress which can provide benefits. Three methods used to cope with stress include:- Aerobic exercise: lowers blood pressure, improves cardiac functions, increases the production of neurotransmitters
- Biofeedback: training to control autonomic responses, meditation, yoga
- Social support: vocalization of thoughts, shared learnings, expressive writing
Can the level of stress resulting from critical life events be measured?
Creating the Social Readjustment Scale involved identifying “stress values” for different major life events. The death of a partner, for example, equated to 100 points, a job loss: 50 points. A truly objective comparison of personal experiences is not possible, due to widely-ranging individual differences in personality.However, there are some characteristics that increase the likelihood of a stress response, since a readjustment to critical life events is complicated by:
- Low degree of predictability
- Low degree of controllability
- Very early break in the biography
- High degree of undesirability
- High personal relevance
The physiological stress reaction: fight or flight

Image: “Altaic Warrior” by Shane Gorski. License: CC BY-ND 2.0
Activation of the sympathetic nervous system: The heart rate, respiratory rate and the blood pressure increase, due to the dominance of the sympathetic system that accrues. It results in vasoconstriction and increased skin conductance. Due to simultaneous inhibition of the parasympathetic nervous system, salivary secretion and gastrointestinal motility decrease.
Constant stress increases the risk of disease
One of the possible consequences of constant psychological stress (for example during the exam period) is summarized by this phrase, which has nothing to do with acute threat situations to the body. It is no longer helpful, but harmful. Prolonged periods of heightened stress increase the risk of cardiovascular and gastrointestinal diseases.Individual-specific and response-specific reactions to stimuli
Physiological stress reactions occur in various organ systems. Usually, we have a “stress spot” that responds in the form of symptoms: a headache, gastrointestinal complaints, muscular tension. This reaction pattern is also referred to as the individual stereotype. On the other hand, some stimuli, such as sudden noise, always lead to the same reaction pattern in humans.Stress models
Exam tip: Preliminary examinations frequently include questions relating to theoretical models, including the following four stress models.The general adaptation syndrome (GAS) by Selye
In 1956, Selye described the best-known model for reaction to chronic stress. He divided this into three phases: the alarm phase, the resistance phase and the exhaustion phase.- Alarm phase: Shock phase (tachycardia, hypotension, hypoglycemia), then contra shock phase (ACTH distribution, increased secretion of adrenal hormones, especially cortisol)
- Resistance phase: Increase in metabolism and the mobilization of energy through ACTH and cortisol, adaptation to the stress status
- Exhaustion phase: The constant distribution of cortisol leads to immunosuppression, and thus to organ damage, psychosomatic disorders and death in the worst case scenario.
Henry’s psychoendocrine stress model
This stress model dating to 1986 involves emotional stress reactions. As a result, stressors can trigger anger, fear or depression. These emotions, in turn, result in a neuroendocrine response pattern.| Emotion | Behavior | Neuroendocrine Reaction Pattern |
| Anger | Fight | Noradrenaline ↑, Testosterone ↑ |
| Fear | Flight | Adrenaline ↑ |
| Depression | Passive subordination | Testosterone ↓, defective regulation of noradrenergic system |
The homeostasis-allostasis-based model
Not everyone reacts to stressors in the same way; the strain depends on the individual’s degree of vulnerability. Homeostasis describes a state of inner physiological, psychological and social equilibrium. Stress threatens this state of balance.Allostasis is the ability to maintain this state despite external stressors. Various genetic factors and acquired reaction patterns are responsible for this (variable) capability.
The Lazarus and Launier coping model: how do I assess a situation?
The coping model by Lazarus refers to this key question in terms of a series of steps.- Primary appraisal: A secondary appraisal only occurs when the stimulus is considered:
- threatening/onerous
- favorable/positive
- neutral/irrelevant
- Secondary appraisal: The individual assesses how to cope with the situation using their own ability to act.
- Coping strategies: Lazarus distinguishes problem-centered strategies (searching for information, direct actions, cognitive coping) and emotion-centered strategies (flight and avoidance, trivializing, distancing or acceptance of responsibility).
- Re-evaluation of the situation (reappraisal): Depending on the coping mechanisms and the demands of the environment, a re-evaluation of the situation takes place in an optimistic or a pessimistic light.
Our behavior and the brain: the electroencephalogram (EEG)
EEG measurements are especially important in psychophysiology and neuromedicine. Electrodes are mounted on the patient’s skull using a standardized schema so that the electrical activity of the brain can be deduced.The spontaneous EEG
The spontaneous EEG displays basic electrical patterns derived by the machine, which can be measured in wake or sleep states without any external influence. Continuously discharging wavebands are represented over a longer time span. EEG patterns differ according to age: in the case of children, the EEG shows lower-frequency waves and, in the waking state, theta and delta waves may also occur.EEG frequency bands
Four types of frequency bands are distinguished in the EEG (memorize this basic knowledge well!):| Alpha waves | Beta waves | Theta waves and delta waves |
| At rest – low-frequency waves: The patient is awake and relaxed with both eyes closed. If alpha waves are derived from several places, it is called a synchronized EEG. | High-frequency waves with low amplitude: The patient opens their eyes or a sensory stimulus occurs that requires attention. If the alpha rhythm is replaced by the beta rhythm, this is referred to as an ‘alpha blockade’ and, at that point, an EEG desynchronization occurs, replacing the previously synchronized EEG. | Low-frequency waves with a high amplitude: In the case of healthy adults, they only occur during sleep, and not in the waking state. |
Changes in the brain’s electrical activity that have a time-based connection to a stimulus are referred to as evoked potentials. They are to be distinguished from the spontaneous EEG. The terms are distinguished in line with the corresponding types of trigger stimuli: visual (light), acoustic (sound) and somatosensory (for example, an impulse). Since the evoked potentials of the spontaneous EEG are superimposed, averaging techniques are used to make them visible.
‘Evoked potentials’ includes slow potential shifts, or, rather, slow brain potentials – the best known being CNV and P300:
- Contingent Negative Variation (CNV): A signal stimulus signals an imperative stimulus that requires a reaction (motoric, for example). A continuous negatively poled event-related potential (ERP) in the EEG (“readiness” to react) follows this signal.
- P300: This comes to the fore during attentional processes. A series of identical tones is interspersed by a deviating tone that requires a reaction. Three hundred milliseconds after the relevant stimulus a positive potential shift occurs.
Note: Negatively poled ERP in the EEG: Indicator for cortical mobilization
Positively poled ERP in the EEG: Positivization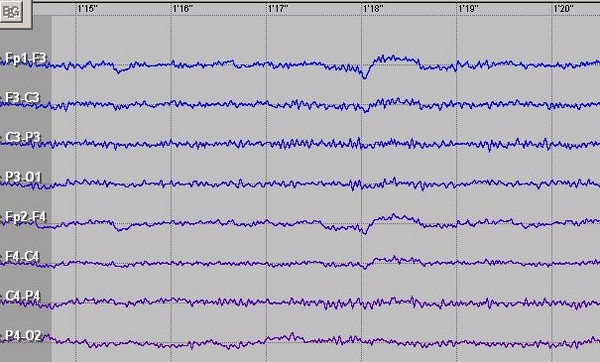
Image: “EEG Beta Activity” by Wojder. License: CC BY-SA 4.0
States of activation and consciousness
Between an alert state of consciousness involving the maximum level of attention and unconsciousness during a coma or deep sleep, there are many shades and variations. Some parameters provide information about the state of consciousness and it is possible for them to be measured subjectively or objectively.Indicators of activation/arousal are:
- respiratory rate ↑, heart rate ↑, blood pressure ↑
- peripheral vasoconstriction
- skin conductance ↑
- concentration ↑
- skeletal muscle tone ↑
- the mental tension felt by the subject
- EEG desynchronization (occurrence of beta waves and alpha-blockade)
- the release of catecholamines ↑
- threshold lowered
The Yerkes-Dodson Law
What level of activation is optimal for good performance? The Yerkes-Dodson Law states that: there is an inverse U-shaped relationship between activation and performance.- An average active level of activation produces optimum performance.
- Easy tasks can be solved well where there is a higher level of activation.
- The more difficult the task, the lower the level of activation.
The orienting response and the defensive reaction
The orienting response (OR) changes the organism’s activation level. This enables the organism to recognize significant stimuli and to respond adequately to them. The OR will be especially high if the stimulus represents a psychologically learned signal (for example, when someone shouts: “Look out!”).The orienting reaction was firstly observed by Pavlov and described as the “What-is-that?-reflex.”
The OR no longer occurs when the stimulus is repeated and provides no new information. The conscious mind becomes accustomed to it, and blanks it out – referred to as: habituation. (Tip: Bear in mind the sound of an ambulance siren and your reaction after one, two and then five minutes.) If the OR increases following a standard stimulus as a result of a short foreign stimulus, this is referred to as a dishabituation.
| Orienting response | Defensive reaction |
| EEG desynchronization; pulse frequency first decreases, before increasing; vasodilation in the head and vasoconstriction peripherally; sweat gland activity increases, skin conductivity increases; mydriasis; increased muscle tone | Defense reaction; target: averting the threat through fight and flight; subjective: fright. |
Sleep: 30% of our lifetime
While sleeping, the organism reduces mental and physical functions to a minimum level of activation (exception: REM sleep). Non-REM sleep stages (1-4) are distinguished from the REM sleep. The duration and rhythm of sleep change over the course of our lives.The amount of sleep needed:
- A newborn sleeps 16-20 hours per day, REM sleep 50%.
- A healthy adult sleeps about 8 hours per day, 20% REM sleep.
- Older people sleep 6 hours or less, REM sleep > 20%.
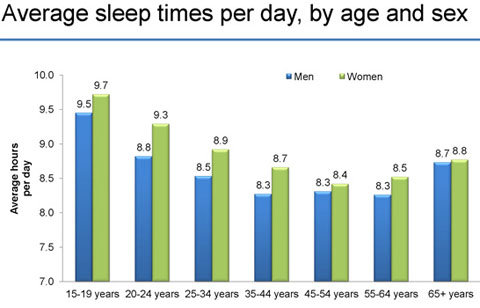
Source: American Time Use Survey, Bureau of Labor Statistics. Data include all persons 15 and older and include all days of the week. These are annual averages for 2012.
It is a biological process that establishes endogenous oscillation in 24 hours. The circadian clock drives these 24-hour rhythms. Chronobiology is the area of science that deals with temporal body rhythms. The light-dark cycle is the most important time-setter for the circadian rhythm.
Excursus: Trials have shown that humans develop a 24-hour rhythm that encompasses sleeping and waking even without the light-based day/night cycle. The anatomical correlate of this biological clock is attributed to the suprachiasmatic nucleus. If this is repressed, any circadian rhythm is nullified, even in the presence of an external time-setter.
The chronobiology of human performance
Memory functions correlate with body temperature: the more difficult the memory task, the more peak performance shifts towards the middle of the day. Peak performance occurs:- at 12:00-13:00 in the case of computational tasks.
- at 14:00-15:00 in the case of linguistic-logical brain teasers.
- and at 03:00 in the case of acoustic reaction-time tasks.
Stages of sleep
A few definitions to help improve understanding of the sleep stages:- REM = Rapid Eye Movement
- Paradoxical sleep: A paradox in that the EEG gives the appearance of “awake,” accompanied by full muscle tone.
- Sleep spindles: High frequency and low amplitude morphologies of the EEG, which mainly occur in stage 2.
- K-complexes: K-complexes are potentials that can be triggered by abrupt and strong stimuli (e.g. thunder and lightning). They can be interpreted as a form of micro-arousals and are characteristic of stage 2 in the EEG.
| Sleep stage | EEG |
| Awake | Alpha waves |
| Falling asleep | Alpha waves ↓, theta waves occur, decreasing muscle tone |
| Light sleep | Theta waves to delta waves, sleep spindles, K-complexes |
| Mid-depth sleep | Transition to delta waves, no longer sleep spindles and K-complexes |
| Deep sleep | Mostly delta waves (slow-wave sleep) |
| Paradoxical sleep (REM sleep) | EEG as in stage 2, rapid eye movement (REM), full muscle tone, occasional muscle contractions (myocloni), cardiac and respiratory rate variability, high dream activity of a very emotional character, possible erection/increase in vaginal blood flow |
NREM STAGE 1
- First stage where one can easily return to the wake stage. Lasts between 1 and 10 minutes. Eyes may roll, and sympathetic activity slows down.
NREM STAGE 2
- Last 20 minutes and accompanied by slowed heart rate, breathing rate and decreased body temperature.
- It becomes harder to wake up and the brain emits larger waves.
- The stage starts 35-45 minutes after falling asleep.
- This is the final stage of standard sleep cycle and takes place after 90 minutes of sleep. The eyes move rapidly in all directions during rapid eye movement. There is increase in heart rate and respiration.
Sequence of sleep phases
In eight hours of sleep, we go through four to six cycles of NREM sleep and REM sleep. The duration of deep sleep phases decreases through the course of the night, and the duration of the REM phase increases.The reason for dreaming is still unknown
You will have already asked yourself this question many times. Various theories address the questions of why we dream and where the contents of dreams originate. The only consensus of dream research is that we probably process information obtained over the course of the day during REM sleep – to the degree that varies greatly from one individual to another – and that transfer of information into long-term memory occurs.Sleep deprivation
In extreme cases, sleep deprivation is lethal. Permanent sleep deprivation makes it impossible for the biological functions of the body to be maintained. You are surely aware of the effects of a brief period of sleep deprivation, from your own experience.- reduced concentration
- a high level of distractibility
- reduced performance in memory-related tasks
- the consequences of several days’ deprivation: hallucinations, EEG sleep phases in the waking state
Sleep disturbances/Insomnia

Dyssomnias: Dysregulation of sleep
Dyssomnias are divided into hypersomnia and hyposomnia.| Hypersomnia (excess sleep) | Hyposomnia (lack of sleep) |
| Sleep apnoea syndrome: Loud, irregular snoring leading to pauses in breathing of up to 10s, especially during REM sleep. Brief awakening due to lack of oxygen and slowed heartbeat which results in massive disruption of sleep structure. During the day, patients are sleepy and unfocused. | Disorders of the sleep-wake cycle: Night-time and shift work, change in time zone/jet lag; (long-term consequences: immunodeficiency, functional and psychosomatic disorders). Resynchronization describes the adaptation of the circadian rhythm to new environmental conditions. |
| Narcolepsy: Compulsive sleep attacks during the day, lasting for several minutes. | Disorders of initiating and maintaining sleep and waking up early, with variable causes e.g., depression. |
Parasomnias
‘Parasomnias’ denotes the group of peculiar phenomena that can occur during sleep. This includes:- somnambulism: sleepwalking
- somniloquy: sleep talking
- pavor nocturnus: nocturnal terror
- bruxism: nocturnal teeth grinding
- nocturnal enuresis: night-time urinary incontinence
Review Questions
The answers can be found below the references.1. A visual stimulus triggers physical reactions. Which of the following is not included?
- Increase in skin conductance
- Increased muscle tone
- Increased respiration
- Raised visual system threshold
- Alpha blockade
- Alpha waves
- Beta waves
- Delta waves
- Gamma waves
- Theta waves



{kind=link}
Comentários
Enviar um comentário