Imaging in Abdominal Trauma
Table of Contents
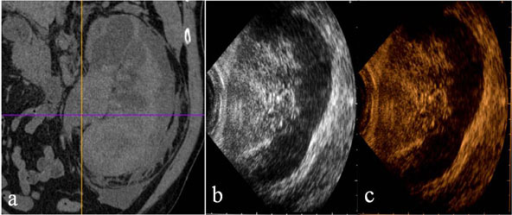
Image: ” Kidney. Contrast-enhanced CT in venous phase (a), US-B-mode (b) and CEUS (c) in a 72 year-old female patient with blunt abdominal trauma. CT shows a renal subcapsular haematoma (a) recocognizable by US B-Mode examination (b) and CEUS corresponding to that of CT.”by Cagini L, Gravante S, Malaspina CM, Cesarano E, Giganti M, Rebonato A, Fonio P, Scialpi M. License: CC BY 2.0
Introduction
Abdominal trauma is classified based on the mechanism of injury into either:
- Blunt abdominal trauma that arises from motor vehicle accidents, fall from a height, assaults and contact sports. It is more common than penetrating abdominal trauma.
- Penetrating abdominal trauma that arises from stab wounds and gunshot wounds. The most commonly injured intra-abdominal organ is the spleen, followed by the liver and the genitourinary organs.
The management of a patient with abdominal trauma involves:
- Primary survey that involves stabilizing the patient via the ATLS protocols.
- Secondary survey which involves history taking of the events that happened. It is performed after stabilization of the patient to prepare for the next stage of management.
- Definitive treatment of an identified cause may take more than 6 months when rehabilitation is needed. Thus, it is never an emergency.
After careful clinical examination and primary survey, the patient is classified as:
- Unstable or transiently responsive patient who needs emergency surgery. This indicates the patient has blood loss more than resuscitation inputs.
- The equivocal patient for whom imaging should be used to exclude life-threatening injuries such as rupture of a major blood vessel.
Current Recommendations for Abdominal Trauma Imaging
Patients who sustained a blunt trauma to the abdomen and are hemodynamically unstable require a rapid evaluation for hemoperitoneum using:
- Diagnostic peritonea lavage (non-imaging)
- Urgent chest radiographs
- Focused assessment with sonography in trauma examination (FAST)
- Pelvic radiograph
On the other hand, a hemodynamically stable patient should receive a multidetector computed tomography (MDCT) scan with IV contrast for the evaluation of visceral and vascular injuries.
Hemodynamically stable patients who have a pelvic fracture, gross hematuria or a red blood cell count in urine of 35,000 or more per high power field should receive a computed tomography cystography after their IV contrast enhanced MDCT to exclude bladder or urethral injury.
Magnetic resonance imaging should be avoided in the acute setting. Magnetic resonance cholangiopancreatography (MRCP) can be used to exclude pancreatic injuries after blunt abdominal trauma but ERCP is superior to MRCP as it is both diagnostic and therapeutic.
Focused Abdominal Sonography for Abdominal Trauma Imaging
Ultrasonography is a rapid, portable, non-invasive and accurate imaging modality, which makes it a good option for abdominal trauma screening. FAST should be only performed by an experienced radiologist. The scan has four windows that represent the main places to look for free fluid on a FAST scan:
- Morrison’s pouch
- Perisplenic area
- Paracolic gutters
- Pelvis
An extended version of the FAST is known as E-FAST and has additional assessment for the hemothorax and pneumothorax, therefore it has two additional windows:
- Bilateral hemithoraces
- Upper anterior chest wall view
FAST can be also performed by an emergency doctor, especially in the United States.
Advantages of using FAST in trauma patients include:
- Rapid and accurate diagnosis of hemoperitoneum.
- Can be repeated for serial examinations without the risks of radiation exposure.
- Integrated into primary patient survey as it is fast and available at the emergency department.
- Non-invasive unlike its predecessor the DPL.
FAST should be limited to looking for hemoperitoneum; the individual evaluation of intra-abdominal organs should not be attempted as it is time consuming and inferior to other imaging modalities such as MDCT.
Computed Tomography in Abdominal Trauma Imaging
Computed tomography is a superior method used for assessment of organ injuries, especially of the pancreas, duodenum and genitourinary system. The main goal of obtaining a computed tomography scan in the blunt trauma patient is to decide whether urgent surgical or angiographical interventions are needed. In contrast to conventional abdominal CT scans, the use of oral contrast with CT in the traumatic patient is not needed.
IV contrast should be always used in the MDCT exam of the patient as it can help in the identification of visceral, vascular or bowel injuries. The lower lung fields and the floor of the pelvis should be included.
Hemoperitoneum on CT
Acute hemoperitoneum has a measured attenuation of 30 to 45 HU on CT. When hemoperitoneum is identified on the CT scan, one should look for the source of bleeding. The location of the hemoperitoneum is dependent on the gravity force and the position of the patient, therefore, it should not be considered when determining the source of the bleed.
Sentinel Clot Sign on CT
It is useful to identify a point of maximum attenuation in the free-fluid collection in the hemoperitoneum as the source of bleeding is usually close to that point. This point is known as the sentinel clot sign.
Active Extravasation on CT
When a hemoperitoneum is identified, the next question is whether active extravasation is happening or not. This can indicate an injury to a major blood vessel, and urgent surgical intervention or therapeutic angiography are usually needed. Active extravasation is confirmed by repeating the CT scan immediately after the first CT scan. If the contrast’s measured attenuation and the size of the hemoperitoneum have increased, extravasation is very likely.
Visceral Injuries on CT
When MDCT is performed, an experienced radiologist should quickly evaluate the different intra-abdominal organs, looking for findings suggestive of an injury while the patient receives their initial primary care.
A systematic approach is needed and different definitions of the different kinds of injuries should be made before one attempts to review an MDCT scan of the abdomen in a traumatic patient.
A contusion is a vague, poorly defined hypodense area in a solid organ. A laceration appears as a linear hypodense area that is irregular compared to a normal fissure. A fracture of a solid intra-abdominal organ is defined as a laceration from one surface to another. A hematoma is oval- or round-shaped and has very high attenuation.
A subcapsular hematoma is a well-defined collection of blood “high attenuation” that appears as an indentation over an organ. Active extravasation is confirmed by performing an immediate repeat CT scan looking for an increase in contrast attenuation or an increase in the size of the free-fluid.
Classification of Various Organ Injuries by CT-Scan
Liver Injuries on CT Scan
The following table summarizes the AAST organ injury scale for the liver.
Spleen Injuries on CT Scan
The following table summarizes the American Association for the Surgery of Trauma (AAST) organ injury scale for the spleen.
Renal Injuries on CT Scan
The following table summarizes the AAST organ injury scale for the kidney.



Comentários
Enviar um comentário