Urethritis (Inflammation of Urethra) — Symptoms and Treatment
Table of Contents
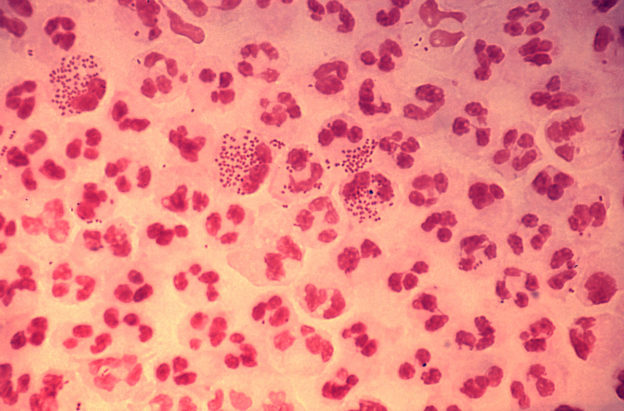
Image: “This low-resolution photomicrograph reveals the histopathology in an acute case of gonococcal urethritis using Gram-stain technique.”by CDC/ Joe Millar – This media comes from the Centers for Disease Control and Prevention’s Public Health Image Library (PHIL), with identification number #4085. License: Public Domain
Definition of Urethritis
Urethritis is a term that means inflammation of the urethra which is usually infectious in etiology. Urethritis is one form of sexually transmitted diseases and can be caused by Neisseria gonorrhoeae or other non-gonococcal etiologies, such as chlamydia, mycoplasma genitalium, trichomoniasis, herpes simplex virus, and ureaplasma urealyticum.
Epidemiology of urethritis
Urethritis is a common condition in the United States, especially among the sexually active population. Approximately, 4 million new cases of urethritis are identified per year in the United States. It can affect both males and females.
When studying the incidence of urethritis, it is better to classify the cases into gonococcal and non-gonococcal urethritis. Gonococcal urethritis is responsible for approximately 700,000 to 1 million new cases per year, while non-gonococcal urethritis accounts for the remainder 3 million cases.
Urethritis carries the risk of ascending pelvic inflammatory disease and approximately 10% up to 40% of women affected by the condition might develop this complication.
Pelvic inflammatory disease is a serious condition that is associated with an increased risk of infertility and ectopic pregnancy. Another common morbidity, especially of non-gonococcal urethritis, is reactive arthritis.
Men affected by the condition can develop urethral strictures and stenosis. If the bacterial pathogens ascend in the affected male patient, he can develop prostatitis, acute epididymitisor can become infertile.
Urethritis is common in both sexes and in all races, but the condition is usually under-reported in women. Homosexual men appear to be at a slightly higher risk of acquiring the condition. The peak incidence is among people in their early twenties.
Etiology of Urethritis
Different organisms can cause urethritis, but this discussion will be limited to organisms classified as sexually transmitted diseases. This infectious urethritis focuses on Neisseria gonorrhoeae, which is a well-understood cause of urethritis in both sexes, but the number of cases related to this bacterium, is declining.
Chlamydia trachomatis, ureaplasma urealyticum and different mycoplasma species are also associated with the development of urethritis. Mycoplasmas are pathogens attributed to urethritis, although they are not like many bacteria as they lack a cell wall and cannot grow on standard media. M. Genitatalium can easily be transferred by sexual contact and accounts for higher cases of urethritis in men than in women.
In women, it can lead to pelvic inflammatory disease, as well as fertility disorders. Urealyticium is a pathogenic cause of NGU in rare cases. C. trachomatis attacks a woman’s cervix and epithelium in a man’s urethra. Viruses such as herpes simplex virus types 1 and 2 can also cause urethritis, but this is a rare phenomenon. Adenoviruses, as well as gardenella vaginalis, can also be potential causes of infectious NGU.
Urethritis not related to sexually transmitted diseases can happen in patients who need recurrent catheterization. This type of urethritis is known as post-traumatic urethritis. Chemical irritation, abnormal growths inside the urethra, as well as autoimmune disease may also cause non-sexual urethritis. Urethritis can also complicate the picture of lower urinary tract infections and cystitis,
Pathophysiology of Urethritis
The different identified organisms for urethritis are known to be transmitted by sexual intercourse. Vaginal and genito-rectal sexual activities carry the risk of transmitting these organisms, but genito-rectal sexual intercourse carries a higher risk.
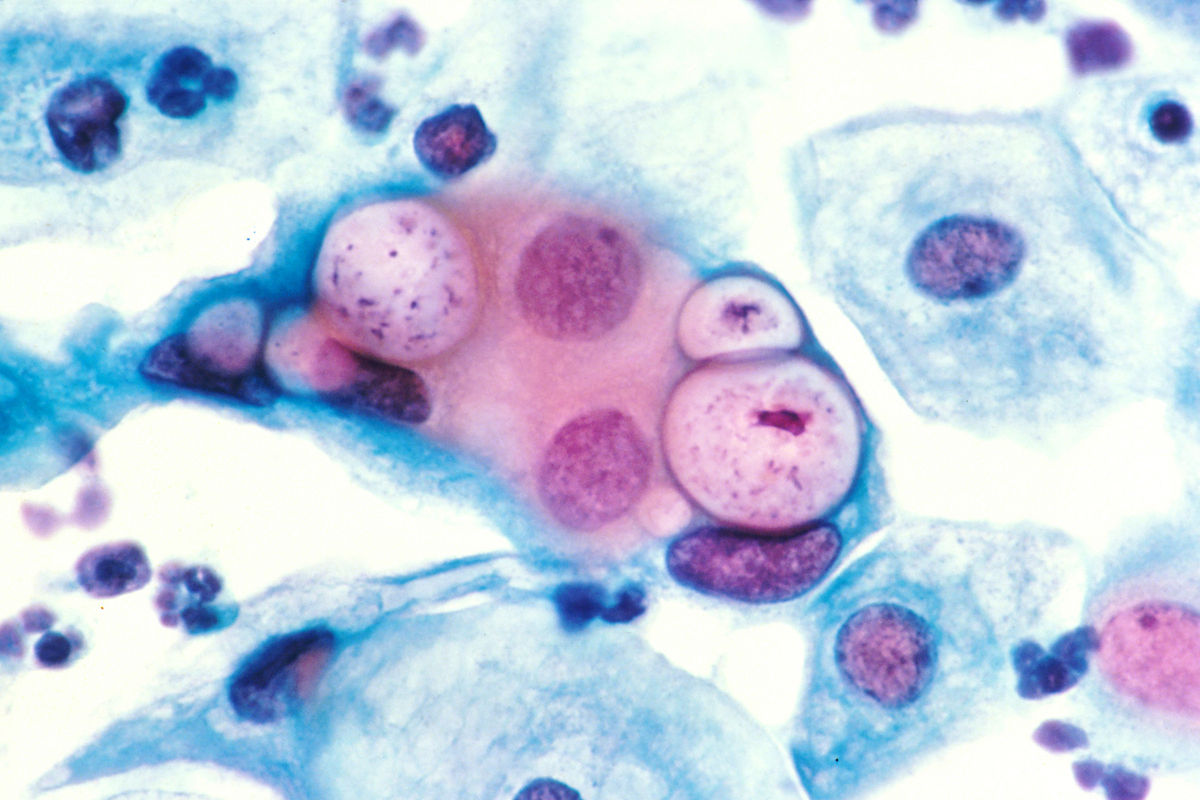
Image: “Human pap smear showing chlamydia in the vacuoles at 500x and stained with H&E.” by http://visualsonline.cancer.gov/details.cfm?imageid=2331. License: Public Domain
Chlamydia is unique because they are obligate intracellular organisms similar to mycoplasma. Because of this, they can be shielded from our immune system. Regardless of the causative organism, an inflammatory response is thought to play the most important role in causing the typical semiology of urethritis.
Because this condition is infectious in etiology, urethritis is commonly found as part of other infectious syndromes, such as epididymitis, orchitis, prostatitis, or urinary tract infections. Patients with untreated urethritis might develop ascending urinary tract infection and bacteremia. This can lead to the development of pneumonia.
Clinical Presentation of Urethritis
The most important role of history-taking in the patient presenting with urethritis is to determine whether the condition is most likely a sexually transmitted disease or not. When taking a sexual history, one should not be judgmental.
There are certain sexual practices that are known to either increase or decrease the risk of acquiring sexually transmitted diseases. For instance, the use of condoms is known to lower the risk of urethritis and sexually transmitted diseases. On the other hand, using chemical spermicides might cause urethral irritation and mimic urethritis.
Another sensitive topic to discuss while taking the history is sexual orientation. Homosexual men are at an increased risk of developing urethritis. Finally, a previous history of sexually transmitted diseases can put the patient at an increased risk of developing recurrent urethritis.
Patients with gonococcal urethritis or chlamydial urethritis are usually asymptomatic, especially women. If the patient has symptoms, they are usually urethral discharge, dysuria, and urethral irritation. Scrotal and testicular pain is also common in men with urethritis.
Menstruating women describe worsening of their symptoms during their menstruation period, similar to pelvic inflammatory disease.
Patients are unlikely to develop fever, chills or other systemic symptoms. Patients who develop arthritis, prostatitis or epididymitis can become feverish and have chills or nausea.
A physical examination can reveal signs of other sexually transmitted diseases, such as ulcersfrom herpes simplex or condyloma acuminatum. Urethral discharge, which can be yellow or green in color, can be seen. Examination should also exclude fever, joint tenderness (especially in the hands and feet), and conjunctivitis.
Diagnostic Workup for Urethritis
The diagnosis of urethritis is based among some clinical and laboratory clues. Purulent discharge from the urethra is a very characteristic finding of urethritis and can be enough to establish a diagnosis. The discharge is yellow or green and occurs in both men and women with the latter having abnormal vaginal discharge and intermenstrual bleeding.
A urethral smear is an important investigation in the diagnostic workup of urethritis. Patients who have infectious urethritis commonly have more than five white blood cells per oil immersion microscopic field on their urethral smear examination.
In contrast to urine analysis for cystitis, one is usually more interested in the first-voided urine and not middle-stream urine in the workup of urethritis. The presence of more than 10 white blood cells per high-power field on microscopy is diagnostic of urethritis.
In the past, treatment options were carefully selected to be either against gonococcal or chlamydial urethritis and not both; therefore, a gram stain was useful in the evaluation and selection of the appropriate antibiotic. Current recommendations, however, state to treat both conditions simultaneously. There have been high rates of resistance in gonococcal urethritis; thus, this step is necessary to avoid a re-occurrence or persistence. Because of this, a gram stain is no longer the recommended test to confirm the diagnosis.
Polymerase chain reaction testing is useful in confirming the presence of neisseria gonorrhoeae, chlamydia, or mycoplasma species. These DNA detection methods allow for the identification of the causative pathogens in urethritis.
Retrograde urethrography should be used only in post-traumatic urethritis, or in patients with recurrent urethritis and suspected urethral strictures.
Treatment of Urethritis
Treatment of urethritis should include the patient and his or her sexual partner/partners.
The treatment of choice for chlamydial urethritis is either azithromycin 1 g orally in a single dose or doxycycline 100 mg two times a day for one week.

Image: “Chemical structure of ceftriaxone, C18H18N8O7S3.” by Edgar181 – Own work. License: Public Domain
Treatment should also cover gonorrhea. Ceftriaxone is an excellent choice for gonorrhea and should be given in a single intramascular dose of 250 mg. It is recommended to combine this with azithromycin to provide coverage against non-gonococcal pathogens as well.
Other possible doses for treatment based on specific treatment include ofloxacin, cefixime and levofloxacin. Metronidazole or tinidazole should be administered for as single doses in case the T. Vaginallis is the cause of the urethritis.
Another important topic that is usually opened during the visit of the patient to the clinic is whether they should abstain from sexual activity while being treated. It is highly recommended to abstain from sexual activity until the patient and the partner/partners have been fully treated to prevent the risk of reinfection.
Patients should be educated about protected sexual activities and the importance of using condoms. Finally, patients should understand that other forms of sexual activity, such as genito-rectal or oral intercourse, are discouraged during the treatment protocol.



{kind=link}
{kind=link}
{kind=link}
Comentários
Enviar um comentário