Ventricular Tachycardia (VT) — Types and ECG
Table of Contents
- Definition of Ventricular Tachycardia
- Epidemiology of Ventricular Tachycardia
- Etiology of Ventricular Tachycardia
- Pathology and Pathophysiology of Ventricular Tachycardia
- Symptoms of Ventricular Tachycardia
- Diagnosis of Ventricular Tachycardia
- Differential Diagnoses of Ventricular Tachycardia
- Therapy of Ventricular Tachycardia
- Progression and Prognosis of Ventricular Tachycardia
- Review Questions
- References
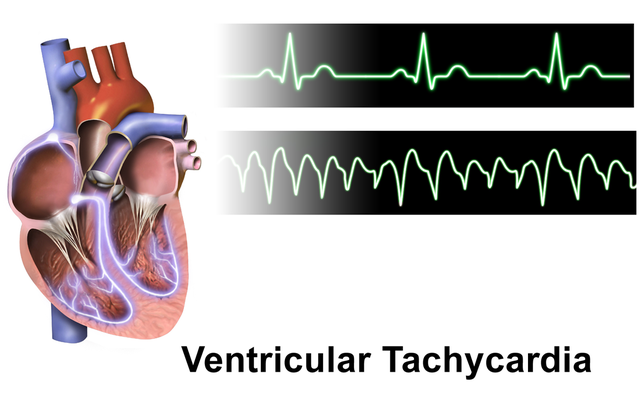
Image: “Ventricular Tachycardia” by BruceBlaus. License: CC BY-SA 4.0
Definition of Ventricular Tachycardia
A ventricular tachyarrhythmia (VT) is any heart rhythm with a rate greater than 100 beats per minute that start in the ventricles. There are many different classifications systems with this type of arrhythmia. One classification system is based on time. A non-sustained VT is short, lasting less than 30 seconds while a sustained VT is longer than 30 seconds.
An additional classification is based on the origin of the ectopic beat. If it repeatedly originates in the same place, it is classified as a monomorphic ventricular tachycardia. If the ectopic beat arises in different places around the ventricle, it is called a polymorphic ventricular tachycardia. Torsade de Pointes is an example of a life-threatening polymorphic ventricular tachycardia.
VTs can be caused by a variety of conditions including:
- Ischemic heart disease
- Electrolyte abnormalities
- Idiopathic (RVOT)
- Structural heart disease
- Medication-induced
There are three important types of ventricular tachyarrhythmias every clinician should be aware of:
- Monomorphic ventricular tachycardia
- Ventricular fibrillation (VF)
- Polymorphic ventricular tachycardia (Torsade de Pointes)
Monomorphic ventricular tachycardia

Image: “Monomorphic ventricular tachycardia” by Glenlarson. License: Public Domain
Monomorphic ventricular tachycardia is a simple, rapid heart rate with an ectopic beat that originates in the ventricle. There is a risk for hemodynamic collapse and sudden cardiac deathin all patients with ventricular tachycardia.
Ventricular tachycardia is further divided into ventricular tachycardia with a pulse and pulseless ventricular tachycardia. In pulseless tachycardia, the heart rate is too rapid, and the rhythm is too uncoordinated to pump blood. This condition should be treated like ventricular fibrillation, and advanced cardiac life support measures should be started immediately, including cardiac monitoring, oxygen, medication, and cardioversion if necessary.
Ventricular fibrillation (VF)

Image: “Ventricular fibrillation” by Jer5150. License: CC BY-SA 3.0
Ventricular fibrillation (VF) is a more severe ventricular tachyarrhythmia. In this arrhythmia, the ventricle rapidly and sporadically beats. The ventricular heart beat is uncoordinated, resulting in immediate hemodynamic collapse. Death is likely within minutes unless advanced cardiac life support measures are started immediately.
Polymorphic ventricular tachycardia

Image: “Torsdade de pointes. The blue line shows the characteristic “twist” around the isoeclectric baseline” by Panthro. License: Public Domain
Polymorphic ventricular tachycardia (Torsade de Pointes) is a ventricular tachyarrhythmia with a rapidly changing rate and rhythm. The rate can change between 150–250 beats per minute and the amplitude also changes when observed by EKG. This arrhythmia may spontaneously revert to normal or progress into ventricular fibrillation.
Epidemiology of Ventricular Tachycardia
Spread of ventricular tachyarrhythmias
VT makes up about half the cardiac mortality rate in the United States. Theincidence increases with age, as the incidence of coronary artery disease increases. Half of all deaths due to coronary artery disease are caused by VF. VF is found more frequently in menthan in women; however, Torsade de Pointes is more frequently found in women.
Etiology of Ventricular Tachycardia
Coronary artery disease & MI
The most common cause of VT is ischemic disease, often after an MI. Scar formation via surgery or infiltrative cardiomyopathy due to systemic inflammatory diseases such as sarcoidosis, amyloidosis, and hemochromatosis also increase the risk to VT.
Coronary artery disease is a major risk factor for VF, and extensive coronary artery occlusion is the most common pathologic finding. Restoring coronary artery flow has demonstrated a reduced risk for VF.
Non-ischemic cardiomyopathy
Dilated cardiomyopathy increases the risk for FV. It is the most common type of non-ischemic cardiomyopathy and is associated with ventricular remodeling and an increased ventricular volume. Hypertrophic cardiomyopathy is frequently a genetic disorder (autosomal dominant) and also increases the risk of FV.
Hypertrophic cardiomyopathy is the most common cause of ventricular fibrillation in patients under 30 years old. Takotsubos cardiomyopathy increases the risk for developing Torsade de Pointes. Takotsubos (AKA broken heart syndrome) is associated with acute heart wall weakness and is often associated with severe stress.
Long QT
Some patients have a naturally long QT interval. The QT interval is measured on an EKG strip from the start of the Q wave to the end of the T wave and represents the depolarization and repolarization of the ventricles of the heart.
Certain medications can also prolong the QT interval (antiarrhythmic, antibiotics such as azithromycin, and psychiatric medications such as haloperidol, methadone, and ziprasidone). A prolonged QT interval can result in polymorphic ventricular tachycardia and Torsade de Pointes. Other conditions can prolong the QT interval such as hypothyroidism. It is also common in type 1 diabetes.
Electrolyte imbalance
Electrolyte imbalance can lead to arrhythmias anywhere in the heart. The heart is most sensitive to low levels of potassium (hypokalemia), calcium (hypocalcemia), and magnesium(hypomagnesemia).
Digitalis toxicity
Digitalis toxicity may result from the excess use or an abnormal reaction to the drug and increases the risk of developing monomorphic ventricular tachycardia.
Pathology and Pathophysiology of Ventricular Tachycardia
Ventricular tachyarrhythmias are abnormal and potentially deadly arrhythmias. They are caused by an abnormal ectopic contraction in the ventricle. The condition may be benign if the ectopic signal is regular and stationary and the cardiac output is maintained, but if the signal moves around the ventricle or if the rate changes rapidly then the arrhythmia could rapidly result in cardiovascular collapse and death. Ischemic change following coronary artery disease or a myocardial ischemic event is the most common cause of VT due to scar formation.
The normal electrical signal slows as it passes through the scar tissue. This pause allows the surrounding ventricle to repolarize. The slowed signal then depolarizes the repolarized ventricular tissue before the supraventricular signal has a chance to pass through the ventricular conduction fibers.
The ectopic beat causes the ventricle to beat very fast (greater than 100 beats per minute) and out of sequence with the atria. The result is a drop in cardiac output and, potentially, sudden death. If the rapid ventricular contraction rate is tolerated, then arrhythmia may cause cardiomyopathy over time.
Torsade de Pointes is closely associated with a prolonged QT interval due to abnormal ion regulation in the cardiac muscles of the heart. Any medications and genetic disorders that result in a prolonged or delayed repolarization that may result in early after depolarization and Torsade de Pointes.
Symptoms of Ventricular Tachycardia
Signs of ventricular tachyarrhythmias
Symptoms include:
- Palpitations
- Lightheadedness
- Syncope
- Sudden cardiac death, especially during ventricular fibrillation
These symptoms often cause the patient anxiety and agitation. Hypoperfusion to the brain may result in lethargy or coma. Additionally, the patient may describe a sensation of neck fullness and difficulty breathing as the venous blood pools and venous pressure increases.
On physical exam patients with VT will show tachycardia. Due to the low cardiac output, they may also show hypotension and tachypnea. VT is also associated with cannon A waves. In this condition the atria and ventricle contract at the same time to produce a strong pressure wave against the mitral and tricuspid valves of the heart. The wave may be visible passing up the jugular vein.
Other symptoms include jaw pain and cough. Other conditions produce a cannon A wave including pulmonary hypertension and complete heart block (third degree AV block).
There may be some short-term or permanent physical changes to a patient after VT has been converted to a sinus rhythm. Displacement of the point of maximal impulse is possible. Any structural heart changes that result in valve disease may produce a murmur. Additionally, an S3 gallop may develop.
Diagnosis of Ventricular Tachycardia
Ventricular tachyarrhythmias are potentially life-threatening. If VT is a concern, then advanced cardiac life support measures should be activated while making the diagnosis.
ECG
An electrocardiogram and physical findings are sufficient to diagnose VT. Tachycardia (greater than 100 beats per minute) with wide QRS complexes (> 120 ms) is sufficient for diagnosis.

Image: “12 lead electrocardiogram of a ventricular tachycardia” by Karthik Sheka, M.D.. License: Public Domain CC BY-SA 2.5
Monomorphic ventricular tachycardia
The ectopic beat is constant, and the QRS wave on ECG will be abnormal but consistent.
Polymorphic ventricular tachycardia
The ectopic beat has many foci in the ventricles and produces a wave form of QRS complexes that appear to twist around an axis. The most common polymorphic ventricular tachycardia condition is Torsade de Pointes or “twisting of the points”.
Laboratory studies
Measure electrolytes for abnormally high or low levels especially potassium, calcium, and magnesium. Measure the blood for medications that may prolong QT or induce VT such as digoxin or tricyclic antidepressants. Measure for recreational drugs such as cocaine and methamphetamines. Evaluate the heart for damage by measuring cardiac enzymes including troponin I and troponin T.
Differential Diagnoses of Ventricular Tachycardia
- Atrial flutter
- Atrial fibrillation
- Premature ventricular contractions
- Myocardial infarction
Therapy of Ventricular Tachycardia
Treatment of ventricular tachyarrhythmias
Ventricular tachycardia treatment can be broken up into short term and long term treatment.
Short term
Ventricular tachycardia may result in hemodynamic collapse and require lifesaving measures to restore a normal sinus rhythm. Signs and symptoms of hemodynamic collapse (if these are present administer lifesaving measures):
- Dyspnea
- Chest pain
- Hypotension
- Altered mental status
First line treatment for hemodynamic instability secondary to ventricular tachycardia is direct current cardioversion.
A stable patient with prolonged monomorphic ventricular tachycardia but no signs of end organ damage should be treated with medication-induced cardioversion with procainamide, sotalol or lidocaine. If there is left ventricular dysfunction, then cardioversion should be undertaken with amiodarone or lidocaine, these antiarrhythmics are preferred because they will not exacerbate left heart failure where procainamide may.
A stable patient with polymorphic ventricular tachycardia should be treated with IV magnesium sulfate, cardioversion, and an antiarrhythmic that will not prolong the QT interval (procainamide and amiodarone are contraindicated).
If ventricular tachycardia is the result of digitalis toxicity treat with anti-digitalis antibody and cardiovert to normal sinus rhythm. If electrolyte imbalance is suspect then carefully and quickly restore electrolyte concentrations to normal and cardiovert.
Long term
The goal of long-term treatment is to prevent ventricular tachycardia with the most effective and conservative treatment available. Treatment options include medication (antiarrhythmics), ablation, and implantable cardioverter-defibrillator implantation. Additionally, evaluate the QT interval and remove and change medications that may unnecessarily prolong the QT interval.
“Treating VT” Image by Lecturio
Progression and Prognosis of Ventricular Tachycardia
Prognosis is dependent on several characteristics but mainly left heart function. Patients with ventricular tachycardia with left heart dysfunction are much more likely to suffer from hemodynamic collapse and sudden cardiac death.
Review Questions
The answers are below the references.
1. A wide QRS tachycardia could result from all of the following but…
- …monomorphic ventricular tachycardia.
- …polymorphic ventricular tachycardia.
- …atrial fibrillation.
- …ventricular fibrillation.
2. Part of the treatment plan for polymorphic ventricular tachycardia should include…
- …IV magnesium sulfate.
- …cardioversion
- …advanced cardiac life support measures.
- All of the above.
3. A mixture of medications that prolong the QT interval can result in…
- …ventricular fibrillation.
- …atrial flutter.
- …atrial fibrillation.
- …Torsade de Pointes.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comentários
Enviar um comentário