Development of the Branchial Arches
Table of Contents

Image: “Human Embryo – Approximately 8 weeks estimated gestational age” by lunar caustic. License: CC BY 2.0
Origin of the Branchial Arches
In the fourth or fifth embryonic week, mesenchymal cells begin to migrate from the neural crest and the paraxial mesoderm into the lateral wall of the digestive tract. Here, they proliferate and thus form four bulges that are on top of each other diagonally, the branchial arches, which are located topographically above the heart and liver. During development, the sixth pharyngeal arch merges with the fourth, while the fifth one is simply rudimentary.
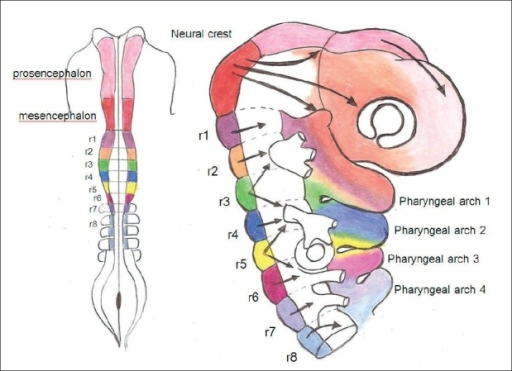
The ectoderm inserts itself between the branchial arches, so that four pharyngeal clefts (sulci branchiales) form. On the inside, four pharyngeal pouches (sacci pharyngeales) form that represent the bulges of the entoderms and are located directly across from the pharyngeal clefts. This is how the branchial arches are separated from each other spatially.
Structure of the Branchial Arches
The branchial arches are metameric structures, meaning that in all branchial arches the same structural elements can be found:
- Cartilage element
- Muscle system
- Branchial arch nerve
- Branchial arch artery
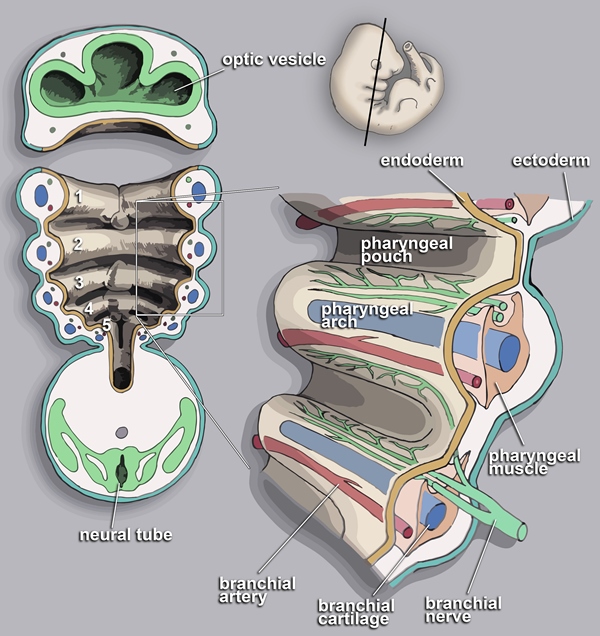
Image: “The Scheme of the Pharyngeal Arch. Re-drawn from the Gray’s Anatomy.” by Loki austanfell. License: CC BY-SA 3.0
Important structures of the skeleton and the musculature in the face and neck area are created subsequently through the development and migration of these elements, with every branchial arch musculature being accompanied by its own branchial arch nerves. While some cartilage elements form important bone structures, some of them degenerate during development.
The pharyngeal clefts, as well as the pharyngeal pouches, are also sites for future organs (see below).
Development of the Face
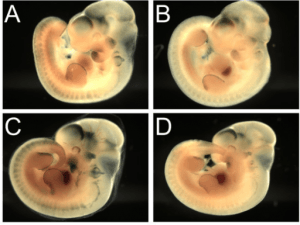
Paired thickenings (placodes) indicate where the nostrils will form on the frontonasal prominence. These deepen into pits with a medial and lateral wall. The maxillary and mandibular process grow towards the midline.
The walls surrounding the nasal pits are not complete — they are open to the mouth. The maxillary process is still separated by grooves from the nasal walls and the mandible. Swellings on the neck show where the ears will form. The eyes are now visible in this frontal view as they move around towards the front. Remember that the whole embryo is growing, though the diagrams do not reflect this.
Swellings on the neck show where the ears will form. The eyes are now visible in this frontal view as they move around towards the front. Remember that the whole embryo is growing, though the diagrams do not reflect this.
The ears become recognisable, though still low down on the neck. The eyes continue to move towards the front and eyelids develop.
The nasal part of the frontonasal prominence begins to fuse wih the maxillary process. The maxillary process begins to fuse with the mandibular process.
Branchial Arch Derivatives
The first branchial arch – mandibular arch
The cartilage element of the first branchial arch is referred to as Meckel’s cartilage. As this is located in the lower jaw (mandibula) system, the first branchial arch is also referred to as the mandibular arch. The largest part of the cartilage degenerates, while another small part forms the two auditory ossicles, the malleus and the incus. The sphenomandibular ligament (ligamentum sphenomandibulare), as well as the anterior ligament of the malleus (ligamentum mallei anterius), originate from the Meckel’s cartilage.
Furthermore, upper and lower jaw bulges originate from the mandibular arch. From the upper jaw bulge, in turn, the malar bone (os zygomaticum), a part of the temporal bone (os temporale, pars squamosa), and the incisive bone (os incisivum), are formed.
From the muscular system of the first branchial arch originates the entire masticatory musculature:
- The masseter muscle
- The temporal muscle
- The medial pterygoid muscles
- The lateral pterygoid muscles
Parts of the muscular system migrate and form muscles for the palate, the middle ear and the bottom of the mouth:
- The tensor veli palatini muscle
- The tensor tympani muscle
- The digastric muscle (anterior venter)
- The mylohyoid muscle (musculus mylohyoideus)

The muscles of the mandibular arch are innervated by the mandibular nerve of the trigeminal nerve (cranial nerve V).
The Second Branchial Arch – Hyoid Arch
From the second branchial arch, important structures of the hyoid bone (os hyoideum)originate, as well as muscles that are attached to it, which is why this arch is also referred to as the hyoid arch. The cartilage originating from it is referred to as Reichert’s cartilage, which forms the third auditory osscile, the stapes. Furthermore, the styloid process of the temporal bone, the cornu minus of the hyoid bone, the cranial part of the hyoid bone body and the stylohyoid ligament originate from it as well.
The mimic muscles (facial musculature) and parts of the suprahyal musculature originate from the hyoid arch muscular system:
- The stylohyoid muscle
- The digastric muscle (venter posterior)
- Furthermore, the stapedius muscle develops as a muscle of the middle ear.

The associated cerebral nerve is the facial nerve (cranial nerve VII).
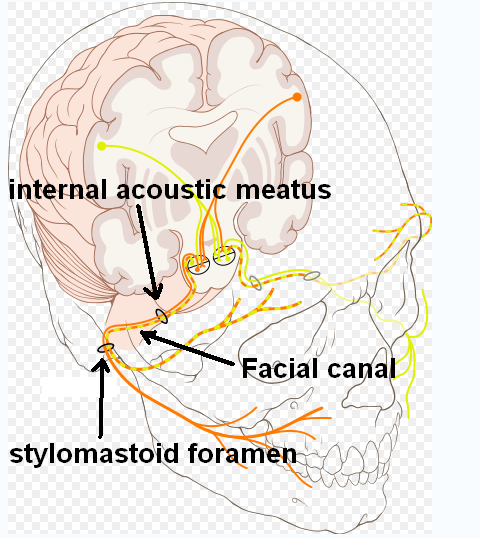
Image: “Cranial Nerve VII 7, with Facial Canal Highlighted” by PhilSchatz. License: CC BY-SA 2.5
The third branchial arch
The cartilage ring of the third branchial arch does not have its own name and forms the caudal part of the hyoid bone body and its cornu majus.
The muscles originating from the third pharyngeal arch are part of the palate, as well as the upper pharynx musculature:
- The palatoglossus muscle
- Partially the palatopharyngeus muscle
- The musculi constrictor pharyngis superior and medius (partially)
- The salpingopharyngeus muscle
- The stylopharyngeus muscle
The nerve of the third branchial arch is the glossopharyngeal nerve (cranial nerve XI).
The fourth branchial arch
The cartilage element of the fourth pharyngeal arch does not have its own name either. Together with the upper part of the thyroid cartilage (cartilago thyroidea), it forms part of the larynx.
From the muscular system of the fourth branchial arch, the cricothyroid muscle develops as the most outer larynx muscle. Furthermore, parts of the middle and inferior constrictor muscles of pharynx and the palatopharyngeus muscle originate from them as well.
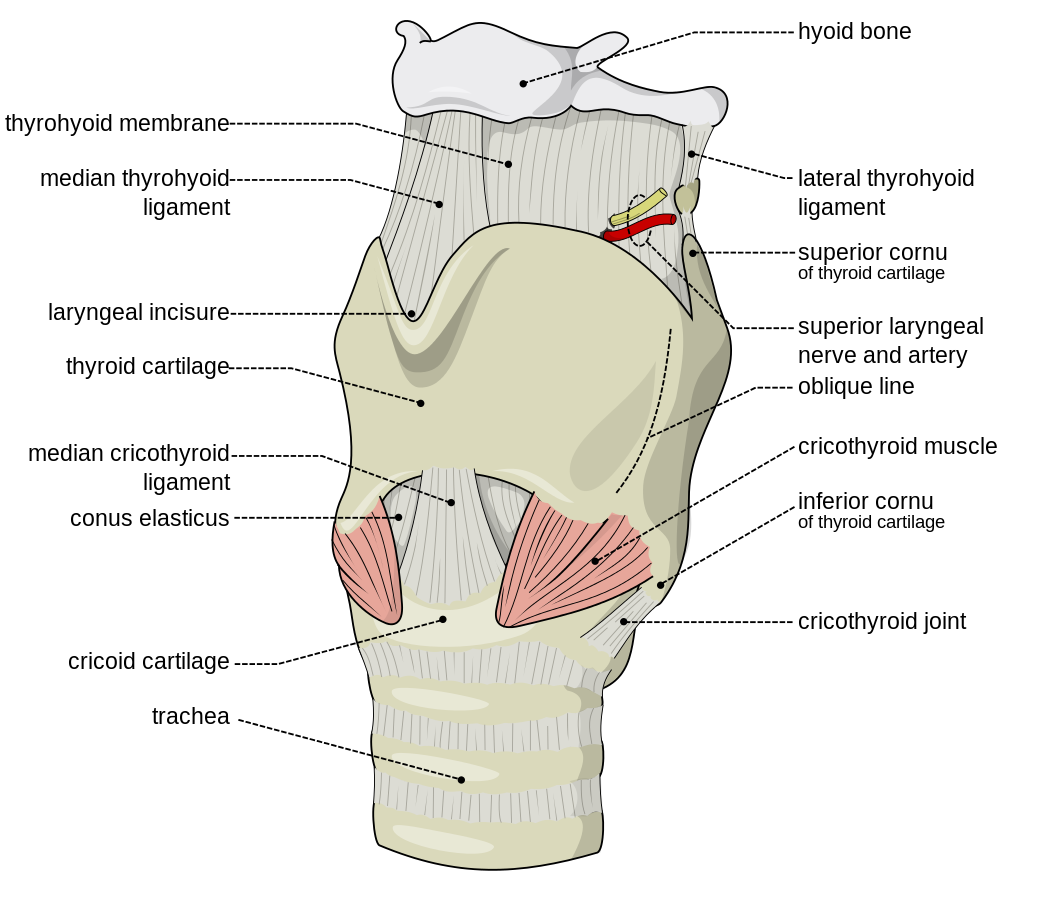
Image: “Larynx – antero-lateral view, with external muscles of larynx visible.” by Olek Remesz. License: CC BY-SA 2.0
The associated nerve is the superior laryngeal nerve ( a branch of the vagus nerve, cranial nerve X).
The sixth branchial arch
The sixth branchial arch merges with the fourth. The remaining cartilages of the larynx skeleton originate from its cartilage ring: the lower part of the thyroid cartilage, the cricoid cartilage, and the arytenoid cartilage.
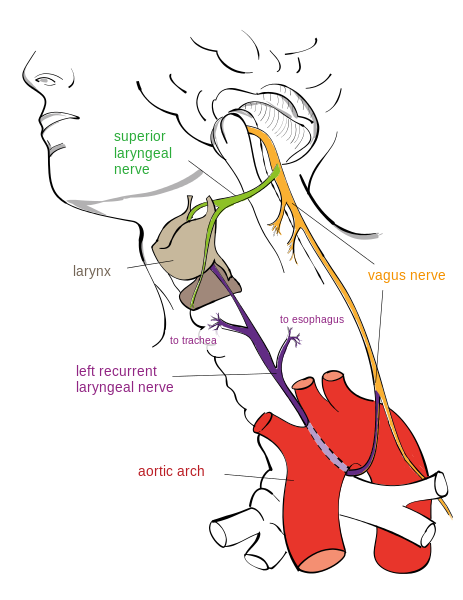
Image: “Drawing of the Left Recurrent Laryngeal Nerve” by Jkwchui. License: CC BY-SA 3.0
From the muscular system, all inner larynx muscles originate, as well as part of the inferiorconstrictor muscle of the pharynx.

The muscles are innervated by the recurrent laryngeal nerve ( a branch of the vagus nerve, cranial nerve X).
Summary of the branchial arch derivatives
In order to provide a better overview, the derivatives of the pharyngeal arches are summarized in the following table:
Derivatives of the Pharyngeal Clefts and the Pharyngeal Pouches
Pharyngeal Clefts
Only one of the four ectodermal pharyngeal clefts (also: pharyngeal/branchial grooves) develops into a definite organ system; from the first pharyngeal cleft develops the external ear canal (meatus acusticus externus), as well as the external part of eardrum (membrana tympani).
The second pharyngeal cleft proliferates strongly and keeps growing caudally until it merges with the epicardial ridge. Hereby, it overlaps the third and fourth pharyngeal cleft, thus acting like a lid for pharyngeal clefts two to four. This way, a kind of deep depression is formed, the cervical sinus, which is lined by the ectoderm. Over the course of development, however, this sinus disappears once more. If this does not happen, lateral branchial cysts may develop (see below).

Image: “Pattern of the branchial arches. I-IV branchial arches, 1-4 Pharyngeal pouches (inside) and/or pharyngeal grooves (outside), a: Tuberculum laterale, b: Tuberculum impar, c: Foramen cecum, d: Ductus thyreoglossus, e: Sinus cervicalis.” by Uwe Gille. License: CC BY-SA 3.0
Pharyngeal Pouches
The pharyngeal pouches grow from the inside toward the pharyngeal clefts and are lined by the entoderm. The recessus tubotympanicus originates from the first pharyngeal pouch. It expands distally into the tympanic cavity (cavum tympani) while the proximal section forms the narrow auditory tube (tuba auditiva).
The auditory tube is also known as Eustachian tube and connects the middle ear with the nose and throat area. Furthermore, the entoderm forms the inner surface of the eardrum (membrana tympani); thus, the first pharyngeal cleft and the first pharyngeal pouch connect with one another and, together, form the structures of the outer and the middle ear.
Through the proliferation of the epithelium of the second pharyngeal pouch, epithelium sprouts form first, followed by the palatine tonsil. The tonsillar fossa, the cavity in which the palatine tonsil is located, originates from the second pharyngeal pouch as well.
In the third pharyngeal pouch, a ventral and a dorsal bulge can be found. While the thymus system develops from the ventral sprout, the dorsal sprout forms the inferior parathyroid gland.
Over the course of the development, the two systems emigrate caudally so that the thymus system winds up in the thorax where it merges with the opposite side. The parathyroid glands migrate to the backside of the thyroid gland. During this migration, it can happen that tissue remnants remain behind.
The fourth pharyngeal pouch also has a ventral and a dorsal sprout. The ventral system, however, does not develop any further and only the dorsal bulge contributes to organ formation. It forms the superior parathyroid glands, which lose the connection to the pharyngeal wall and attach themselves to the thyroid gland above the inferior parathyroid glands.
The fifth pharyngeal pouch is frequently attributed to the fourth one. It forms the ultimobranchial body, which is the origin of the calcitonin producing C cells (parafollicular cells) of the thyroid gland; the ultimobranchial body is incorporated into the thyroid gland.
In order to provide a better overview, the pharyngeal pouch derivatives are summarized in the following table:
Branchial Arch Arteries
Each branchial arch has its own branchial arch artery (also: aortic arch, pharyngeal arch artery), which means that there are six aortic arches altogether, which partially degenerate and which are never present all at the same time. From them, the large vessels close to the heart develop. They originate in the aortic root and lead into the two paired dorsal aortae, which merge caudally into the descending aorta. In the beginning, the branchial arch arteries are still symmetrical, which is, however, lost over the course of the development (see below).
The first and the second branchial arch artery degenerate for the most part and only leave behind small amounts for the development of the maxillary artery (first pharyngeal arch artery) and the stapedial artery (second pharyngeal arch artery). Contrary to that, the third pharyngeal arch artery remains intact. While the proximal sections form the common carotid artery, the distal sections form the internal carotid artery together with parts of the dorsal aorta.
From the fourth branchial arch artery, the defined aortic arch (arcus aortae) emerges from the left, and the proximal section of the right subclavian artery (arteria subclavia dextra) emerges from the right. A fifth aortic arch is not set up in most cases. Just as asymmetrically developed is the sixth pharyngeal arch artery, which is also referred to as pulmonary arch. To the left, the ductus arteriosus Botalli develops; to the right, the truncus pulmonalis as well as the proximal part of the pulmonary artery. By the time the sixth branchial arch artery has fully developed, the first and second have already disappeared.
Malformations during the Development of the Branchial Arches
Lateral branchial fistulas and cysts

Image: “Laterale Halszyste” by Wellenschik. License: CC BY-SA 3.0
Should the cervical sinus persist, lateral branchial fistulas can form, with the opening of the fistula being at the anterior edge of the sternocleidomastoideus muscle and leading into the supratonsillar fossa. Branchiogenic cysts do not have an opening; they are elastic to the touch and can be red and painful. Diagnostically, they are to be separated from a branchiogenic carcinoma. Therapy consists of surgical removal because otherwise relapses can occur.
Goldenhar Syndrome (Oculo-auriculo-vertebral Dysplasia)

The Goldenhar syndrome, also referred to as hemifacial microsomia, represents a combined malformation of the first and second branchial arch leading to different asymmetrical facial anomalies:
- Malformations of the outer ear (i.e., small or missing outer ear (microtia, anotia))
- Ocular tumors or dermoids
- Missing eye
- One corner of the mouth is elevated
- Flat temporal bone
- Malformations of the spine (i.e., fused vertebrae)
The reason for this disease is unknown.
Review Questions
Solutions can be found below the references.
1. Which association between the branchial arch and branchial arch derivative is not true?
- First branchial arch: Meckel’s cartilage
- Second branchial arch: Styloid process
- Third branchial arch: Greater horn of hyoid bone
- Fourth branchial arch: Stapedial muscle
- Sixth branchial arch: Vagus nerve
2. What develops from the first pharyngeal pouch?
- Palatine tonsil
- Eustachian tube
- Thymus
- Inferior parathyroid gland
- Ultimobranchial body
3. Which statement regarding aortic arches is true?
- All six aortic arches exist at the same time.
- The peripheral arteries of the lower extremities originate there.
- The third and fourth aortic arch completely degenerate.
- The ductus arteriosus Botalli is a derivative of the fourth pharyngeal arch artery.
- The truncus pulmonalis is a derivative of the sixth pharyngeal arch artery.
4. Lateral branchial cysts…
- …are residues of the thyroglossal duct.
- …have the same cause as medial branchial cysts.
- …are always malignant.
- …must be removed surgically.
- …are located in the area of the trapezius muscle.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comentários
Enviar um comentário