Lactation and Breastfeeding
Table of Contents

Structure of the Female Breast
An adult woman breast is an exocrine gland overlying the pectoral muscles and is composed of 15-20 separate compartments called lobes that are further divided into lobules. Each lobe has its own ductal system called the lactiferous duct that drains out at the nipple. The main parts of the female breast are:
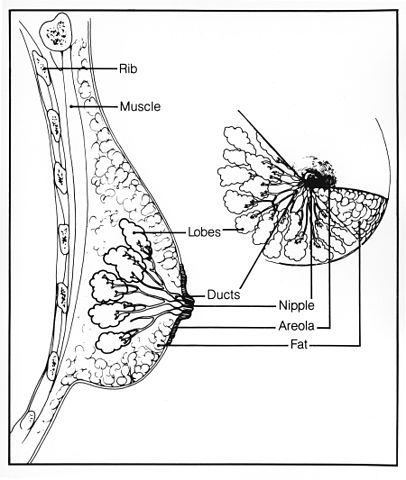
Image: “Breast structure.” by Susan Spangler (Illustrator) – This image was released by the National Cancer Institute, an agency part of the National Institutes of Health, with the ID 1810. License: Public Domain
- Lobules, which are the milk-producing glands and are composed of several alveoli. The alveoli are lined by cuboidal epithelium and surrounded by the myoepithelial cells, which have a contractile ability.
- Lactiferous ducts form the channel passage for milk from alveoli to the nipple.
- Stroma is composed mainly of fatty tissue and ligaments which surround the lobules, ducts, lymphatic and blood vessels.
- The lactiferous ducts empty into the nipple, which is the central part of the areola. The areola is the dark-colored skin consisting of sweat glands. The figure shows the structure of the female breast.
Development of the Breasts
Breast formation begins during fetal development when there is thickening of the chest area to form the mammary ridge or milk line. When the female baby is born, nipples and the breast duct system are present. It is up to puberty when the breast further develops under the influence of female sex hormones. This is a part of secondary sexual characteristics in females. Although the diet of an individual also influences the breast development, hormonal stimulation plays a major role. This explains a remarkable increase in breast size during pregnancy.
Under normal physiological conditions, the process of lactation and milk production starts after parturition, which again is under hormonal control. These hormones are discussed in detail below:
Breast changes during pregnancy
Breast are believed to achieve their final phase of development under the influence of pregnancy hormones. Thus, the hormones are important in:
A high amount of estrogen is released by the placenta during pregnancy
- Estrogen causes the development and branching of the ductal system
- It causes an increase in stromal tissue
- Deposition of fat in the breasts resulting in an overall increase in weight and size. The average increase in the weight of breasts during pregnancy is 2 pounds.
The role of progesterone includes the initial development of the ductal system. Progesterone works synergistically with estrogen. Its main role in breast development is highlighted below:
- There is an overall growth of the lobules and budding of the alveoli
- The alveoli gain secretory function
- Its function is further enhanced by the action of growth hormone, prolactin, insulin, and glucocorticoids.
Breast changes during menopause
At the age of 45, the hormonal environment changes to favor low levels of estrogen. This reduces the amount of glandular tissue in the breast and the available tissue is dehydrated and inelastic.
The above factors cause the breast to shrink and loose shape. This is commonly referred to as “sagging”. It is important to note that this is irreversible even with hormone replacement therapy once it sets in.
Initiation of lactation and the role of prolactin
As mentioned previously, the breasts are able to produce a sufficient amount of milk after delivery. However, the initiation of lactation occurs in the fifth week of pregnancy under the influence of prolactin hormone. Prolactin is secreted by the anterior pituitary gland. Its blood levels begin to rise in the fifth week of pregnancy until delivery, at which its level is 10 times greater than in a non-pregnant female.
The lactogenic effect of prolactin is supported by a hormone produced by the placenta calledhuman chorionic somatomammotropin.
The secretory effect of prolactin is inhibited by estrogen and progesterone during pregnancy, even though a few milliliters of fluid are secreted every day. This is a physiological response as, during pregnancy, the fetus gets all the nutrients from the maternal blood and does not require to be breastfed.
The fluid which is secreted in the last few days of pregnancy, and just before parturition, is called colostrum. It contains exactly the same amount of lactose and protein as breast milk, yet has no fats. The rate of production of colostrum is 100 times less than the rate of the production of breast milk.
Soon after the birth of the baby, the inhibitory role of estrogen and progesterone diminishes and the process of milk production starts. In 1-7 hours postpartum, copious amounts of milk are produced under the lactogenic effect of prolactin.
As mentioned above, other hormones also play their role in the production of milk as they provide the required amino acids, fatty acids, glucose, and calcium.
The basal level of prolactin soon becomes equal to that of a non-pregnant female. If the mother feeds her newborn at regular intervals, every time she nurses him, neuronal signals go to the hypothalamus, increasing the level of prolactin to 20 folds. This is called a prolactin surge and is required for milk production.
Prolactin is therefore required to keep the mammary glands functional. If the mother stops feeding her child, the prolactin surge does not occur and the milk production stops. However, if she continues feeding, the milk production continues for a few years postpartum, but the quantity may decline over 8-9 months.
Role of hypothalamus in milk production
Hypothalamus is known to stimulate the pituitary hormones. However, in case of prolactin, it has an inhibitory role. If the baby suckles the nipples, neuronal signals are sent to the hypothalamus and the inhibitory effect on secretion of prolactin is lost. Thus, prolactin is secreted by the pituitary gland leading to milk production. If there is an injury to the hypothalamic-hypophysial system, the inhibitory response is permanently lost causing an increase in prolactin secretion. There are two factors secreted by the hypothalamus:
- Prolactin inhibitory hormone (PIH) which remains dominant most of the time and inhibits prolactin secretion. Dopamine, a PIH tends to decrease prolactin by 10-folds.
- Prolactin releasing factor (PRF), which has an intermittent effect in releasing prolactin.
Prolactin, on the other hand, is thought to decrease the production of gonadotropin releasing hormone (GnRH) by the hypothalamus. This eventually suppresses the production of follicle stimulating hormone (FSH) and luteinizing hormone (LH) by the pituitary gland.
Nursing mothers, therefore, do not ovulate as follicles do not undergo maturation and development. This occurs in approximately half of the nursing mothers. With continuous feeding, the pituitary gland overcomes the inhibitory effect and starts producing FSH and LH. Breastfeeding, therefore, acts as a natural contraceptive.
Role of oxytocin in the secretion of milk
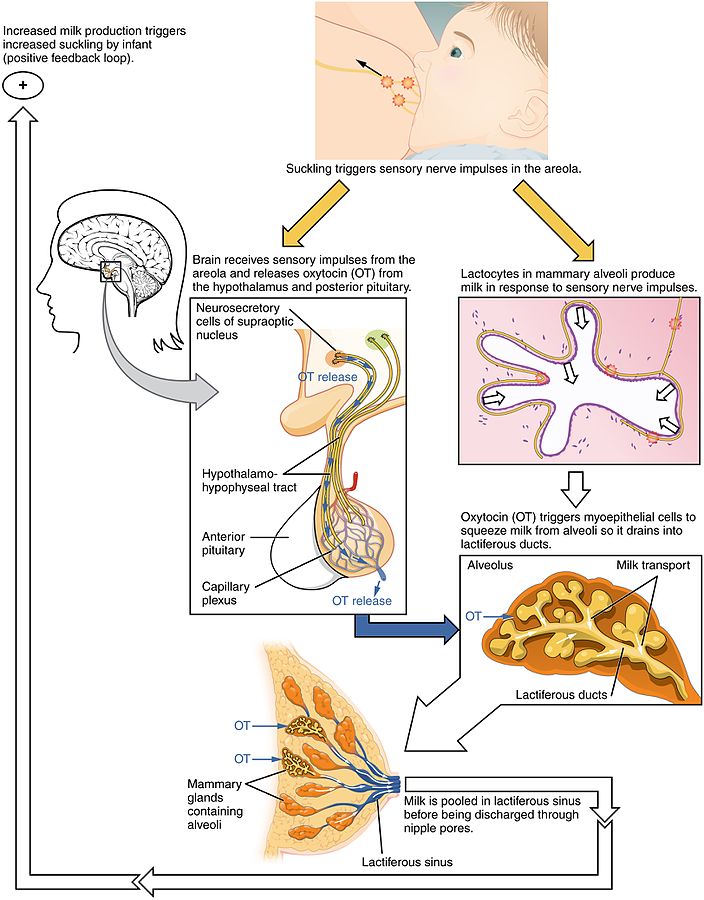
Although the milk that is produced is continuously being secreted in the alveoli, it has to travel through the ductal system to reach to the baby’s mouth. When the baby suckles the nipples, initially he is not sucking any milk. Sensory signals traveling through the somatic nerves reach the spinal cord and finally to the hypothalamus, which secretes another hormone called oxytocin.
Oxytocin travels in the blood to reach the myoepithelial cells surrounding the outer wall of the alveoli, causing them to contract. This increases the pressure inside the alveoli to 30mmHg and forces milk into the ductal system.
Oxytocin and prolactin are secreted simultaneously and, after 30 minutes of suckling, milk starts to flow in the ductal system. This is known as the ‘let down’ process, well demonstrated in the figure.
Several other factors also influence the release of oxytocin, such as the sound of baby crying, fondling the baby by the mother and otherpsychogenic factors. Therefore, undisturbed puerperium is essential for successful nursing.
Sucking Reflex
The sucking reflex is a primitive instinct present in all newborn mammals. It is linked to the rooting reflex and allows the baby to suckle anything that comes into contact with the roof of the mouth. At four months the involuntary response changes into a voluntary conscious action. The infant may suckle anything that touches his/her mouth but that is not an indication for hunger but a response. It comprises of two components:
- Expression: when the nipple is placed between the child’s lip and palate, he will move the tongue to press the nipple.
- Milking: the child will move his tongue away from the nipple towards the areola, to be able to swallow the milk expressed.
Composition of Breast Milk
Breast milk is the primary source of nutrition for the newborn. It not only contains the required nutrients but also protects the baby against infections as his immune system has not been developed yet. As per the World Health Organization (WHO) guidelines, a mother should breastfeed her child up to two years.
Human breast milk consists of the following components:
- Total fats up to 4.2 g/mL with poly unsaturated fatty acids of 0.6 g/mL
- Total protein up to 1.1 g/mL. It includes casein, lactalbumin, and immunoglobulins IgG and IgA, albumin, and lysozyme and beta lactoglobulin
- Lactose is the major carbohydrate present up to 7 g/mL. Other oligosaccharides are 0.5 g/mL
- Minerals such as calcium, iron, phosphorus, sodium, potassium, and chlorine are also present
- Folate and Vitamin C content is remarkably greater in human breast milk when compared to goat’s or cow’s milk
Galactorrhea
Galactorrhea is the spontaneous flow of milk from the mammary glands, unrelated to pregnancy or breastfeeding. It can occur in both males and females irrespective of their age.
Hormonal irregularities such as hyperprolactinemia, elevated levels of thyrotropin releasing hormone (TRH) and thyroid stimulating hormone (TSH) are frequently associated.
History of drug intakes such as methyldopa, opioids, antipsychotics, selective serotonin reuptake inhibitors (SSRIs), oral contraceptive pills (OCPs), and behavioral causes need to be ruled out in a patient with galactorrhea.
Certain pituitary adenomas also produce a high level of prolactin in the blood. As mentioned above, prolactin inhibits ovulation and is one of the causes of infertility.
Agalactorrhea or Lactation Failure
It is a medical condition in which there is an insufficient production of milk or an absence of the ‘let down’ reflex in response to suckling. The mother is therefore unable to breastfeed her newborn baby.
It can be investigated by doing blood prolactin levels, which are usually low in such cases. It can be treated with galactagogues such as domperidone, certain antipsychotics, TRH or TSH. Lactation failure with normal to high level of prolactin may be because of Sheehan’s syndrome or lymphocytic hypophysitis.
Review Questions
The correct answers can be found below the references.
1. A 46-year-old male presented to his family physician with a complaint of discharge from the nipples, along with off and on low-grade fever. He has complaint of a headache and vomiting early in the morning. On examination, he has HR 105/min, RR 28/min, BP 140/90 mmHg and discharge from both the nipples more at night. CBC shows hb 10 mg/dl, normal TLC with lymphocytosis. Local examination showed no swelling or tenderness. Which of the following could be the most probable cause to these complaints?
- Hirsutism
- Mastitis
- Pituitary adenoma
- Hyperthyroidism
2. A 30-year-old fresh mother came to her family gynecologist with a complaint of insufficient breast milk production. On examination, there was no deformity of the breasts and they are normally developed. The child is also active and his sucking reflex is satisfactory. The child was born by a C-section at the start of the 9th month of gestation. Which of the following medication would you advise?
- Phenobarbital
- Domeperidone
- Acetazolamide
- Misoprostol



{kind=link}
{kind=link}
LifeVoxel.AI is used in detecting breast cancer and reducing diagnostic errors by 85%.
ResponderEliminarRIS PACS
RIS PACS Software