Alcoholic Hepatitis, Alcoholic Cirrhosis & Non-Alcoholic Fatty Liver Disease (NAFLD)
Table of Contents
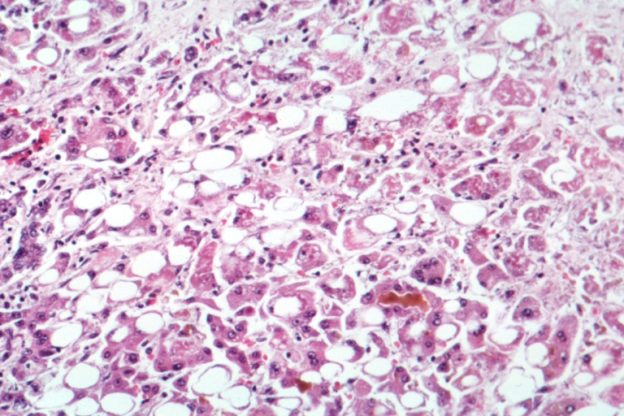
Image: “Microscopy of the liver showing evidence of alcoholic hepatitis”. The original uploader was Countincr at English Wikipedia – Transferred from en.wikipedia to Commons, License: CC BY-SA 2.5
Definition
Hepatitis is the inflammation of the liver, or more specifically, inflammation of the liver cells. There are different types of hepatitis, which may occur due to multiple reasons, ranging from consumption of contaminated food to certain sexual practices to alcohol overdose. Here, however, we will study a particular form of hepatitis in depth, known as alcoholic hepatitis.
Alcoholic liver disease presents as three forms, (1) fatty liver, (2) alcoholic hepatitis, and (3) cirrhosis.
Alcoholic hepatitis is the inflammation of the liver cells due to excess alcohol consumption over an extended period of time. Between 10 and 20% of alcoholics develop alcoholic hepatitis. Though this disease is still curable if detected in the early stages, however, if alcohol consumption is not tapered off and the disease is not treated properly, it may worsen. Alcoholic hepatitis left untreated can even lead to additional health issues such as cirrhosis or complete liver failure. Alcoholic hepatitis is usually accompanied by fatty liver disease, which is another disease which may be caused by excess intake of alcohol

Image: “Liver steatosis (fatty liver disease) as seen on CT” by James Heilman, MD. – Own work, License: CC BY-SA 3.0
The fatty liver disease occurs when there is an abnormal accumulation of fat in the liver cells. Though it is often studied in relation to alcohol consumption, it actually occurs in two forms: alcoholic fatty liver disease and non-alcoholic fatty liver disease (NAFLD or NASH). Fatty liver is seen in >90% of daily/ binge drinkers.
While the cause of the alcoholic fatty liver disease is clear, non-alcoholic fatty liver disease occurs due to many reasons other than alcohol consumption. These reasons include problems such as diabetes, high blood pressure and a high level of blood fats, i.e. obesity. This type of fatty liver disease also eventually results in cirrhosis if not treated properly.
Cirrhosis, which is the end result of both alcoholic hepatitis and non-alcoholic fatty liver disease, is a condition where the liver fails to function properly due to long-term damage. This damage is usually in the form of either alcohol or the causes of non-alcoholic fatty liver disease. This condition can even further lead to many complications and even graver diseases such as liver cancer.
Risk Factors
- Alcohol:The major and most obvious risk factors for alcoholic hepatitis are the quantity of alcohol one consumes and the duration of intake. Though the exact amount which puts someone at risk is not known, it is vaguely calculated to be around seven glasses of alcohol every single day for a period of at least 20 years.
- Gender:Apart from alcohol consumption, gender is also a risk factor, because the way alcohol is processed inside the body also plays an important role. This is why women tend to be at a greater risk of developing alcoholic hepatitis than men. The threshold for developing alcoholic liver disease in men is >14 drinks per week, whereas it is >7 drinks per week in women.
- Obesity:High levels of alcohol, accompanied with overweight’s, make someone more vulnerable to not only alcoholic hepatitis but also to fatty liver disease, which may progress to cirrhosis in the long run. High cholesterol levels also put patients at greater risk of developing a non-alcoholic fatty liver disease.
- Genetic factor:Many studies deduce that there is a link between the genetic component and alcohol-induced liver diseases.
- Environmental factors: Although it is hard to separate the genetic factors from the environmental ones, it is seen that factors such as race and ethnicityhappen to play a part too. For example, African-Americans and Hispanics seem to be at greater risk of alcoholic hepatitis.
- Existing diseases: Pre existing diseases, such as chronic infection with hepatitis C virus, metabolic syndrome, type-2 diabetes, hypothyroidismor underactive pituitary gland, can increase the risk of developing NAFLD.

Image: “Macroscopic image of micronodular (liver) cirrhosis caused by alcohol consumption” by Amadalvarez – Own work, License: CC BY-SA 4.0
Pathophysiology
Alcoholic cirrhosis
The damaged hepatocytes undergo abnormal repair, which leads to fibrosis, which is the scarring and hardening of the liver and its cells. Extensive fibrosis disrupts the structure of the liver, causing the liver to shrink.
Non-alcoholic fatty liver disease
This results when the uptake of lipids by liver overwhelms the mechanisms for triglyceride disposal, leading to accumulation of fat within hepatocytes . This increased delivery of fatty acids to the liver, causes the liver to swell up and malfunction. Insulin resistance is created, which leads to alcoholic hepatitis. NAFLD is also said to be the leading cause of cryptogenic cirrhosis, with varying degrees of fibrosis.
Clinical Features of Alcohol-Related Liver Diseases
Alcoholic Fatty Liver Disease
- Can be asymptomatic
- Hepatomegaly
- RUQ discomfort
- Nausea
Alcoholic Hepatitis
- It can be asymptomatic
- Lack of appetite
- Weight loss, also as a result of a change in appetite
- Yellow color in skin and eyes, jaundice oricterus
- Fever
- Fatigue or a general sense of weakness and lack of energy
- Nausea and vomiting
- Pain in the abdomen, accompanied by tenderness. Especially pain specifically in the upper right abdomen
- Swollen abdomen due to excess fluid accumulated there
- Mental confusion or problem in thinking straight.
Alcoholic Cirrhosis
In addition to the above features, some additional ones include:
- Edema, i.e. building up of fluid in the legs, thus swelling them
- Redness in palms
- Easy bruising, abnormal bleeding at even the slightest of cuts
- In men, smaller testicles.
Non-Alcoholic Fatty Liver Disease
In addition to all of the symptoms of alcoholic hepatitis, a few other features are unique to NAFLD:
- Itching
- Red spider-like blood vessels throughout the skin
- Swelling of legs.
Investigations and Diagnosis of Alcohol-Related Liver Diseases
Clinical manifestations and laboratory features are enough to identify alcoholic hepatitis in a patient with a long-term heavy alcohol drinking. Heavy alcohol use is defined as drinking more than 100 g of alcohol per day for more than 20 years, providing the absence of other common causes of acute hepatitis.
History
A thorough research needs to be done to understand the patient’s drinking habits – how often the patient drinks and whether they can function without it and other such questions to gaugethe body’s dependency on alcohol.
Patient with alcoholic hepatitis is typically 40 to 50 years old of age, with a history of a daily heavy alcohol drinking “more than 100 g per day”, for more than 20 years, which might occur in response to stressful situations in patient’s life.
Physical examination
This will help in bringing about symptoms such as tender hepatomegaly, jaundice, and fever. In patients with advanced diseases, a physical examination can also bring about signs of portalhypertension, ascites, and a bruit might be heard over the liver.
Ascites may occur due to either portal hypertension, or obstruction of portal venous flow as a result of hepatic cells swelling.

Image: “Cirrhosis with ascites (marked)” by James Heilman, MD – Own work, License: CC BY-SA 4.0
The presence of stigmata of chronic liver disease, such as ascites, palmar erythema, spider angiomata, gynecomastia and others, suggest underlying liver cirrhosis.
Blood tests
1. Liver tests abnormalities:
- Gamma-glutamyl transaminase (GGT):
- Lone elevation (with/without alanine transaminase [ALT] and aspartate aminotransferase [AST]) is a possible sign of occult alcohol abuse.
- AST: ALT ratio (liver transaminase):
- ALT is more specific for the liver than the AST because AST is also found in the liver, cardiac and skeletal muscle, kidneys, and lungs
- Both AST and ALT are usually moderately elevated (< 500 int.unit/mL), (<400 IU/mL) with or without elevated GGT in alcoholism.
- AST: ALT ratio ≥ 2 AST: ALT ratio ≥ 1 is associated with alcohol abuse (alcoholic hepatitis).
- Elevated serum bilirubin (> 5 mg/dL)
- Other liver markers derangements: Hypoalbuminemia , Coagulopathy and modest elevations of Alkaline phosphate.
- Mean corpuscular volume (MVC):
- A larger size of red blood cells (due to nutritional deficiencies) that resembles macrocytic anemia (MCV > 100 fl)
Laboratory investigations to rule out other causes of acute hepatitis should be done, such as:
- Anti-hepatitis A IgM
- Hepatitis B surface antigen, anti-hepatitis B core IgM
- Anti-hepatitis C virus (HCV) antibodies, hepatitis C RNA.
Imaging tests
- Tests such as Trans-abdominal U/S, MRI, and CT scansare carried out to get visuals of the liver which provide valuable input in understanding the state of liver functioning.
- The imaging tests may reveal parallel tubular structures in the liver. (? Referring to venous collaterals). Portal vein flow reversal, ascites, and intraabdominal venous collaterals on ultrasound indicates serious/irreversible liver injury.
Liver biopsy
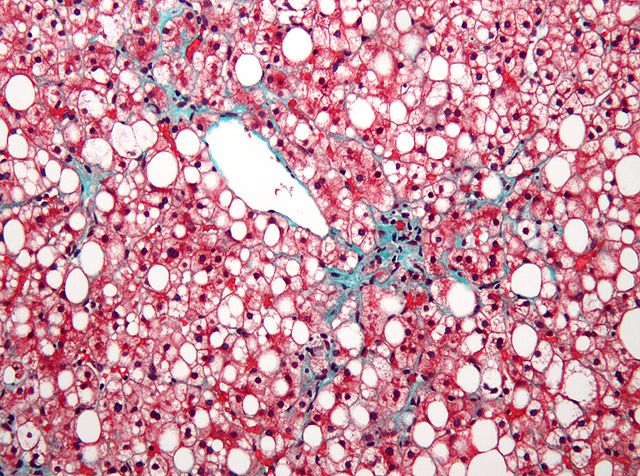
Image: “Micrograph of non-alcoholic fatty liver disease (NAFLD)” by Nephron – Own work, License: CC BY-SA 3.0
Liver biopsies are not necessary and depend on the severity of the disease. A biopsy of the liver is useful in diagnosing the full extent of the liver damage which helps in understanding the severity of both the fibrosis and the level of inflammation.
Furthermore, it helps in evaluating other possible liver diseases such as the fatty liver disease which may accompany alcoholic hepatitis. Liver biopsies are vital not only for alcoholic hepatitis but also for non-alcoholic fatty liver disease, to confirm the accumulation of fat in the liver.
Differential Diagnosis of Alcoholic Hepatitis
Alcoholic hepatitis should be differentiated from other causes of acute hepatitis, in which the striking features to identify alcoholic hepatitis are:
- Heavy alcohol drinking
- AST: ALT ratio of ≥2, which is rarely noticed in other causes of acute liver disease.
Acute hepatitis
The differential diagnosis of acute hepatitis is wide and includes the following:
- Acetaminophen toxicity
- Drug-induced liver injury/idiosyncratic drug reactions (including herbal supplements and illicit drugs)
- Non-alcoholic steatohepatitis
- Acute viral hepatitis (hepatitis A, hepatitis B, hepatitis C, hepatitis D, hepatitis E, herpes simplex virus, Ebstein-Barr virus, cytomegalovirus)
- Ischemic hepatitis
- Budd-Chiari syndrome
- HELLP (hemolysis, elevated liver enzymes, low platelets) syndrome
- Acute fatty liver of pregnancy
- Wilson´s disease
- Autoimmune hepatitis
- Alpha-1 antitrypsin deficiency
- Toxin-induced hepatitis (e.g., mushroom poisoning, carbon tetrachloride).
High aminotransferases can also be noticed other diseases such as:
- Muscle diseases
- Thyroid disease
- Celiac disease
- Adrenal insufficiency
- Anorexia nervosa.
Treatment of Alcoholic Hepatitis
The management of alcoholic hepatitis includes several measures:
- Abstinence from alcohol
- Treatment of alcoholic withdrawal
- Hemodynamic and nutritional support
- Medical treatment
Abstinence
Patients at only the initial stages of liver diseases can still control further deterioration by abstaining from the cause of all the damage. This means abstinence from alcohol in the case of alcoholic hepatitis, and abstinence from obesity causing products in the case of NAFLD. Abstinence will also result in prevention from cirrhosis, in both the cases.
Excessive alcohol drinking for a long time makes the patient at risk of withdrawal symptomswhich also should be treated promptly.
Alcohol abstinence and the general supportive measures are adequate in the treatment of mild to moderate alcoholic hepatitis. Medical treatment with glucocorticoids is not beneficial in the treatment of mild or moderate alcoholic hepatitis.
Hemodynamic and nutritional support
Patients with alcoholic hepatitis should be hydrated because poor oral intake associated with the presentation may result in dehydration.
Overhydration should be avoided in patients with a chronic liver disease with signs of cirrhosis because this may increase the size of the ascites, increase the risk of hyponatremiaand predispose to variceal hemorrhage.
Nutritional support with adequate calories, proteins, vitamins, and minerals is important to improve liver function.
Lifestyle changes, loss of body weight and dietary modification in NAFLD patients can improve serum aminotransferases and hepatic steatosis.
Medical treatment
Medical treatment with glucocorticoids (prednisolone 40 mg/day for 28 days, followed by gradual tapering of the dose over 2 to 4 weeks) is indicated in patients with severe alcoholic hepatitis (MELD score>20) (Harrison’s 20/e) in addition to the general supportive measures.
For non-alcoholic fatty liver disease, there is no set approved medicines but the anti-inflammatory medicines like Aspirin, Ibuprofen, Naproxen Sodium, Celecoxib etc. are often prescribed. The drugs currently being studied for NAFLD include Metformin, Pioglitazone, Vitamin E, omega-3 fatty acids. The approach to NAFLD management focuses on improvement of risk factors for NASH i.e., obesity, insulin resistance, metabolic syndrome, and dyslipidemia.
Surgical considerations
When the disease becomes acute, there is a greater risk of complete liver failure. In such cases, the only treatment offered is a liver transplant. However, surgery too, is complicated, as the mortality rate in alcoholic patients is high. Nevertheless, surgery is the last resort for acute stage disease despite prevailing complications.
Counseling and therapy
Referral of patients to alcohol counselors/alcohol treatment programs is a routine process in the management of patients with alcoholic liver disease. Therapy helps many patients break the habit of drinking or help them fight obesity. Counseling helps patients fight the disease before it gets any worse and also helps keep the patients and their symptoms under observation. There are also many support groups, the most famous being Alcoholics Anonymous, which help patients abstain from alcohol.
In order to deal with NAFLD, there are not many counseling methods which have progressed. The newest emergence is the anti-fibrotic therapy to help patients suffering from non-alcoholic fatty liver disease, but it too is still in its initial stages.
Prognosis
The presence of ascites, variceal hemorrhage, deep encephalopathy, or hepatorenal syndrome predicts a poor prognosis. Patients with severe alcoholic hepatitis who are critically ill have 30-day mortality rates >50%. Model for End-Stage Liver Disease (MELD) score ≥21 is associated with high mortality in alcoholic hepatitis.
Review Questions
The correct answers can be found below the references.
1. What is the characteristic liver enzymes pattern in alcoholic hepatitis?
- AST: ALT ratio ≥ 2
- AST: ALT ratio = 2
- ALT: AST ratio ≥ 2
- ALT: AST ratio = 2
2. What is the definition of heavy alcohol drinking?
- More than 100 g per day, for more than 20 years
- More than 20 g per day, for more than 30 years
- More than 100 g per day, for more than 10 years
- More than 200 g per day, for more than 20 years
3. Medical treatment with glucocorticoids is indicated in addition to the general supportive measure in the treatment of what?
- Mild alcoholic hepatitis
- Moderate alcoholic hepatitis
- Non-alcoholic fatty liver disease
- Severe alcoholic hepatitis



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
nice
ResponderEliminar