Flu (Influenza) — Symptoms and Treatment
In Lecturio :). Patients with influenza virus infection can present with cough, fever, sore throat and body aches. Influenza virus infections can be caused by type A virus, the most virulent, type B virus, or type C virus.. The diagnosis can be clinical but laboratory confirmation tests are also available and recommended. Treatment is usually supportive but antiviral therapy can help alleviate the symptoms and shorten the duration of the illness if started within the first 48 hours of the onset of symptoms.
Table of Contents
Are you more of a visual learner? Check out our online video lectures and start your infectious diseases course now for free!
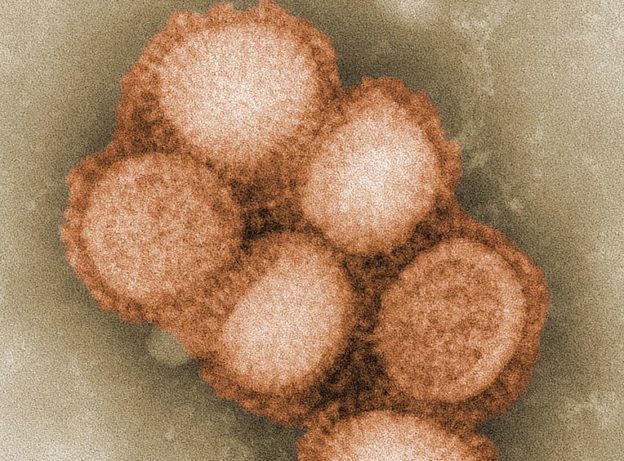
Image: “This colorized negative stained transmission electron micrograph (TEM) depicted some of the ultrastructural morphology of the A/CA/4/09 swine flu virus.” Photo Credit: C. S. Goldsmith and A. Balish, CDC. License: Public Domain
Overview
Influenza, or the flu, is one of the most common infectious diseases in the world. It is responsible for epidemics and has a wide range of symptoms ranging from a mild upper respiratory tract infection to death depending on the patient’s immune status.Seasonal variations of the virus are responsible for more deadly strains such as the Spanish flu, swine flu and avian flu. Additionally, it is important to note that the symptoms of the disease commonly overlap with other viruses such as adenovirus and parainfluenza virus.
Epidemiology of Influenza Virus Infections
The Influenza virus is responsible for a significant number of infectious diseases all over the world. Severe illness has been reported to affect up to 5 million people annually and the influenza virus is responsible for approximately 500,000 deaths per year.In the United States, the influenza virus is estimated to be responsible for at least 3000 deaths per year. However, this figure is based on statistical modeling as influenza is not a reportable disease.
H1N1 influenza strain is responsible for the swine flu and hit the United States in 2009. It was responsible for approximately 500 deaths. The Avian flu virus is responsible for 375 deaths worldwide. It seems that these strains of the influenza virus are more fatal compared to the common strain but fortunately are less likely to spread and so far the number of reported cases seems to be low.
Certain groups of people are known to be at an increased risk of mortality and morbidity from influenza virus which includes those older than 65 years, children younger than 18 years of age, and the immunocompromised.
Etiology of Influenza Virus Illnesses
There are three main types of the influenza virus that are responsible for human disease, influenza virus type A, B or C. In terms of pathogenicity, influenza virus type A is the most pathogenic while type C is the least virulent.| Characteristics | Influenza A | Influenza B | Influenza C |
| Natural host range | Humans, swine, equine, birds, marine mammals | Humans only | Humans and swine |
| Epidemiology | Antigenic shift and drift | Antigenic drift only | Antigenic drift only |
| Clinical manifestations | May cause large epidemics with significant mortality in young persons | No pandemics; confined to older adults and immunocomprised | Mid disease without seasonality |
Pathophysiology of Influenza Virus Infection
The influenza virus has eight different genome segments composed of RNA. Two virulence proteins are hemagglutinin (H) and the neuraminidase (N). There are 18 subtypes of hemagglutinin (H1- H18) and 11 subtypes of neuraminidase (N1-N11). The type of hemagglutinin and neuraminidase is part of the naming convention for different types of influenza virus. Hemagglutinin is responsible for the binding of the virus to the respiratory epithelium while the neuraminidase is implicated in the virus spread to other cells.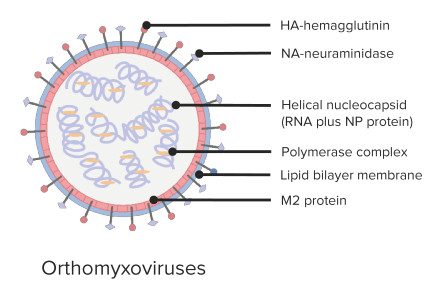
The influenza virus genome is constantly in a state of flux. One reason is that its RNA-dependent RNA polymerase does not check for errors during transcription, unlike DNA polymerases. Therefore, the chance of transcription errors increases and as a result, different strains and variants of the same virus occur. These mutations are the result of genetic drift, the slow change of the virus due to mutations over the course of years. Additionally, whole genome segments can be swapped out during infection. A bird type influenza virus and a human type influenza virus can both infect an animal, usually a pig. If this occurs at the same time, there is a chance these two viruses could infect the same cell at the same time resulting in a shuffling of their genome segments and a new and potentially deadly virus. This is called genetic shift, a rapid and potentially lethal change in the viruses genome.
Transmission to humans can happen from direct contact with infected animals such as in swine and avian flu or from human–to–human contact. Human–to–human spread is airborne and the virus usually spreads via aerosols when an infected patient coughs or sneezes.
Once a person is infected the prodrome period can last anywhere from one day to one week. The prodrome period can last anywhere from one day to one week. An infected person is contagious about one day before symptoms become evident. Once the virus enters a new host, respiratory epithelium dysfunction occurs and inflammatory mediators are released. As a result of this, systemic features of influenza virus infection ensue.
Clinical Presentation of Influenza
In most cases of influenza virus infection, the symptoms start suddenly.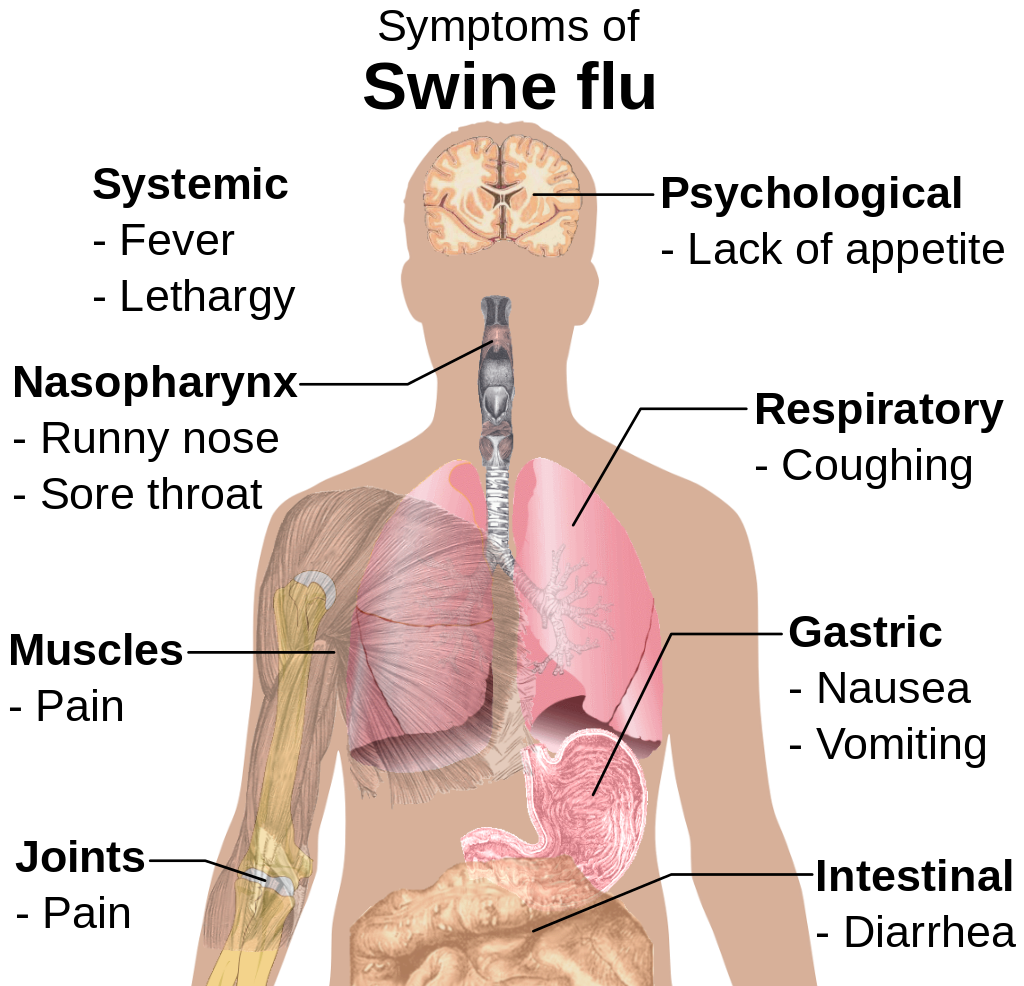
Image: “Main symptoms of swine flu.” by Mikael Häggström. License: Public Domain
Most patients seek medical attention because of the severe sore throat which can last up to 5 days. These symptoms are usually milder in people who have received the annual influenza vaccine.
Physical examination confirms the presence of fever, tachycardia and pharyngitis. The eyes can be red and watery. Patients can have a normal chest examination, but in few cases wheezes can be heard which are usually focal. The patients look tired.
Additionally, patients can be dehydrated because of the fever and the inability to drink fluids due to the sore throat.
Complications of Influenza Infection
Patients with influenza can develop primary influenza pneumonia. Such patients usually progress to severe cough, develop dyspnea and become cyanotic.Pregnant women, patients older than 65 years, and those with cardiovascular disease are at risk of developing primary influenza pneumonia.
Additionally, patients with influenza are at risk of developing secondary bacterial pneumonia. The most commonly implicated pathogens are Staphylococcus aureus, Streptococcus pneumoniae, and Haemophilus influenzae. Patients with secondary bacterial pneumonia appear severely ill, have a productive cough, develop leukocytosis and have lung infiltrates on chest x-rays.
Avian flu carries the highest risk of progression to adult respiratory distress syndrome and is responsible for a significant number of hospitalizations related to influenza.
Diagnostic Work-up for Influenza
While laboratory investigations do not provide any specific findings for the diagnosis of influenza, certain patterns have been identified. Patients usually have leukopenia and lymphopenia unless they develop secondary bacterial pneumonia. Patients can also have hypoxemia.Rapid diagnostic tests of influenza are available and they show good accuracy but somewhat limited sensitivity.
The QuickVue Influenza A+B test can provide a confirmatory result in 10 minutes while the Zstat Flu test takes 20 minutes to show the result. These tests can have less accuracy because of the frequent genetic changes in the influenza viruses, therefore, their specificity should be checked annually.
More recently, the Alere I Influenza A and B test was approved, which is based on accurate molecular testing. The results can be achieved within 15 minutes and the test is believed to be more reliable compared to the currently available rapid diagnostic tests.
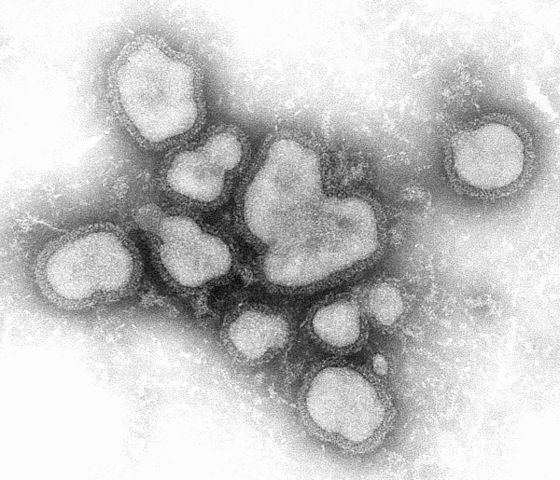
Image: “Transmission electron micrograph, negative stain image of the influenza A virus.” License: Public Domain
Recently, a reverse-transcriptase polymerase chain reaction test was approved for the detection of influenza virus infection. This test can differentiate between influenza type A and B viruses, can classify “type A viruses” by subtypes based on the H and N genes and is able to detect the highly pathogenic avian virus (H5N1).
The inflammatory response to influenza virus infection is different from bacterial pneumonia. Therefore, some have advocated the use of a testing panel that is based on interleukin 10 to distinguish between influenza and other viral or bacterial pneumonias. Influenza was found to be associated with a significantly higher interleukin-10 blood concentration compared to other etiologies of pneumonia and patients had an average of 88.69 pg/mL IL-10.
Imaging studies are needed in patients presenting with symptoms of possible complications or in high-risk populations such as the elderly. Chest x-rays can show multiple and diffuse infiltrates – a picture consistent with adult respiratory distress syndrome. Patients with diffuse lung infiltrates that are consistent with adult respiratory distress syndrome should be screened for possible avian influenza virus infection.
Treatment of Influenza
Our current understanding of genetic shift and drift in the influenza virus allows us to anticipate the most likely epidemic strain this season. Therefore, influenza virus vaccination becomes a possibility and it has been recommended for all people aged 6 months or older. Annual vaccination against influenza virus not only prevents the disease in most patients, but can also alleviate the symptoms of influenza if the person develops the disease that year.
Image: “Tamiflu.” by en:User:Moriori – Photo taken for Wikipedia by Moriori Transfered from English Wikipedia; en:Image:Tamiflu.JPG. License: Public Domain
These antivirals can help by alleviating the symptoms, prevent complications in patients at risk, making the disease duration shorter, and decrease mortality in more severe strains such as the avian influenza strain. In fact, current recommendations are to use antivirals for up to 6 days after the onset of the symptoms in people with confirmed avian influenza infection hoping to lower mortality.
These treatments carry higher costs and a significant adverse effects’ profile. Therefore, the decision to prescribe them should be based on the individual case. Accordingly, antiviral therapy should be used only in a select population of patients who are severely ill, require hospitalization, are at risk of complications, and in any patient who present with symptoms that started in less than 48 hours.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comentários
Enviar um comentário