Total Anomalous Pulmonary Venous Connection (TAPVR) — Pathophysiology and Surgery
In Lecturio . Patients with a total anomalous pulmonary venous connection (TAPVC) have abnormally draining pulmonary veins that drain into the right atrium or the systemic venous circulation. Patients are usually symptomatic early in life. If left untreated, the condition is usually fatal. Echocardiography and magnetic resonance imaging are helpful in the confirmation of the diagnosis. Surgical correction for redirection of the pulmonary veins drainage to the left atrium is the mainstay of treatment.
Table of Contents
- Definition
- Overview of the heart circulation
- Epidemiology of Total Anomalous Pulmonary Venous Connection
- Pathophysiology of Total Anomalous Pulmonary Venous Connection
- Clinical Presentation of Total Anomalous Pulmonary Venous Connection
- Diagnostic Workup for Total Anomalous Pulmonary Venous Connection
- Treatment of Total Anomalous Pulmonary Venous Connection
- References
Are you more of a visual learner? Check out our online video lectures and start your pediatric cardiology course now for free!
© Lecturio GmbH
Definition
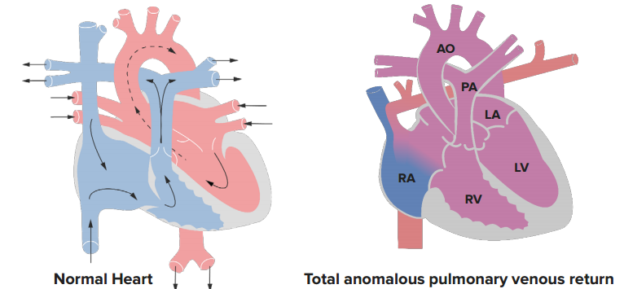
Total Anomalous Pulmonary Venous Connection (TAPVC) is a congenital heart abnormality that is characterized by abnormal blood flow where the pulmonary veins drain into the right atrium or the systemic venous circulation. For the patient to survive during the fetal and the neonatal period, the foramen ovale between the two atria must be patent.Overview of the heart circulation
Blood from the peripheral circulation enters the heart through the vena cava into the right atrium where it is then taken to the right ventricle and later pumped through the pulmonary circulation into the lungs for oxygenation.Oxygenated blood travels through the pulmonary vein into the left atrium and left ventricle where it is pumped to the peripheral circulation via the aorta.
In TAPVC, the oxygenated blood either empties into the right atrium or the pulmonary artery; thus, two separate circulations are present leading to poor vascularization of peripheral tissues and cyanosis.
For the patient to survive during the fetal and the neonatal period, the foramen ovale between the two atria must be patent to allow for surgical correction of the defect.
Epidemiology of Total Anomalous Pulmonary Venous Connection
The prevalence of TAPVC is estimated to be around 6.8 per 100,000 in live births. The incidence of TAPVC in patients with congenital heart defects is estimated to be around 1.5%.Sex differences are still under debate. While the Baltimore-Washington Infant Study showed a very small female predominance, other studies have shown a significant male predominance of up to 3:1 male to female ratio.
Pathophysiology of Total Anomalous Pulmonary Venous Connection
Patients with TAPVC have a volume overload on the right atrium and right ventricle. When the foramen ovale is restrictive, right atrial pressure increases and patients might develop venous systemic and pulmonary congestion. Additionally, blood flow to the pulmonary circulation is usually increased and patients are at risk of developing pulmonary arterial hypertension.The blood flow to the left atrium and left ventricle is dependent on the patency and restrictiveness of the foramen ovale; therefore, the left side of the heart receives blood volume that is less than normal and the cardiac index is usually reduced.
Patients with TAPVC might have normal blood oxygenation by increasing the pulmonary blood flow by three to four times.
Clinical Presentation of Total Anomalous Pulmonary Venous Connection
The presentation of TAPVC is dependent on whether the patient has pulmonary vein obstruction or not. Patients who have the site of drainage of the pulmonary veins below the diaphragm or supracardiac are very likely to have some degree of pulmonary venous obstruction. This group of patients is usually symptomatic during the first days of life. They might develop tachypnea, tachycardia, and cyanosis.Pulmonary hypertension might develop very early in this group of patients which is characterized by a worsening of the cyanosis. If left untreated, the neonate usually dies within the first month of life. A physical examination usually reveals a prominent right ventricular impulse. The heart is usually not enlarged and the apex beat is not displaced. Liver enlargement is commonly seen in this group of patients. Finally, patients might have an increased pulmonary component of the second heart sound.
Patients who do not have pulmonary vein obstruction usually have milder symptoms. Failure to thrive and recurrent respiratory tract infections, similar to large atrial septal defects presentation, are commonly seen. Patients might also have difficulties while feeding.
A physical examination usually reveals a wide split in the second heart sound but with a normal pulmonary component. Patients might be cyanotic, but this is usually less commonly seen compared to the previously described cohort of patients.
If for some reason, the foramen ovale becomes more restrictive to blood flow, pulmonary hypertension might develop. In that case, the patient might develop signs and symptoms suggestive of right-sided heart failure, i.e. systemic and pulmonary venous congestion.
Diagnostic Workup for Total Anomalous Pulmonary Venous Connection
The determination of the level of peripheral blood oxygenation is essential in the diagnostic workup of the neonate or infant who presents due to TAPVC. Patients are also at risk of developing acid-base imbalances and their arterial blood gases should be examined.The main finding of TAPVC on electrocardiography is that of right ventricular hypertrophy. A chest X-ray might show a normal heart with diffuse reticular patterns from the hilum. Patients with an unobstructed pulmonary venous return to the right heart might have cardiomegaly on their chest X-ray due to right atrial and right ventricular enlargement. Patients with pulmonary congestion might have pulmonary edema.
Echocardiography usually provides definitive evidence for the diagnosis of TAPVC. Color Doppler studies are usually indicated to evaluate the pulmonary veins and to see if they drain within the left atrium. Additionally, echocardiography can help in the delineation of the restrictiveness of the patent foramen ovale. Fetal echocardiography can be also used in establishing the diagnosis in a high-risk fetus, i.e. a positive family history of congenital heart disease in general or TAPVC in particular.
Magnetic resonance imaging is superior to echocardiography in that it is not operator dependent and can also help with the evaluation of the associated lung disease such as lymphatic congestion.
Patients with multiple intracardiac and extracardiac sites of pulmonary venous return might benefit from cardiac catheterization.
Treatment of Total Anomalous Pulmonary Venous Connection
If early surgical correction is not possible, an atrial septostomy might be performed, especially if the patient has a restricted foramen ovale. Patients with severe obstruction to pulmonary venous return might benefit from the placement of a stent until definitive surgical correction is possible.Surgical treatment for TAPVC has one main goal, to restore the normal relationship between the pulmonary veins and the left atrium. Patients with extracardiac TAPVC should have their common pulmonary vein opened and then connected side to side to the left atrium.
Patients who have intracardiac TAPVC, i.e. draining into the right atrium or the coronary sinus, should undergo a partial resection of the atrial septum. After the resection of the atrial septum, the patients should get a new atrial septum that is the site of the entrance of the pulmonary vein, i.e. to direct the pulmonary veins to the left atrium. In other words, the left atrium now consists of the normal left atrium in addition to part of the right atrium where the pulmonary veins are draining.
After directing the pulmonary veins to the left atrium, the foramen ovale should be closed. Patients with multiple sites of extracardiac drainage should undergo a side to side procedure to connect the left atrium with the common pulmonary artery, followed by the ligation of the other pulmonary veins.
Postoperatively, the patient might develop episodic pulmonary hypertension which might have an adverse effect on the cardiac output. In that case, nitric oxide should be used for its pulmonary dilator effects. Extracorporeal membrane oxygenation might be needed in very ill patients with poor oxygenation of the blood.
Newborns who are very ill to undergo surgical intervention should receive diuretics to relieve pulmonary edema, and surgical relief of the obstructed TAPVC should be offered as soon as possible.



Very impressive article! The blog is highly informative and has answered all my questions.
ResponderEliminarTo introduce about our company and the activities, E-Healthcare Lists is one of the global suppliers of healthcare mailing list & email list. At E-Healthcare Lists, you get a list of Pulmonologist mailing list which makes your prospecting easy.
I am very much happy to share to every viewers that is reading this,I want to inform the whole public of how I got help for my herpes, I wanted this since 6 months ago, I have also taken treatment from some doctor,few weeks back I came on the net to see if I will be able to get any information as to cure my herpes, on my search I saw various testimony of people who was helped by a great man called Dr Akhigbe and without any hesitation, I contacted him, I wrote to him and and he guided me, I asked him for solutions and he started the remedies for me and indeed 3 weeks after I started using the medicine, I was completely happy as it worked for me.I went to the hospital for check up and indeed I was declared negative from my disease, and I also waited again for two weeks and went back to another hospital for check up to be fully sure and to my great surprise I was still declared negative, and I decided to share this great opportunity to those people out there fighting this sickness, You can contact him now for your medicine to cure your diseases, contact his Email; drrealakhigbe@gmail.com or Whatsapp +2349010754824 website. hpps:drrealakhigbe.weebly.comDr Akhigbe also cure diseases like..
ResponderEliminarHIV, Herpes , Cancer, Chronic Disease, Asthma , Parkinson's disease, External infection, Als, progeria, common cold, multiple sclerosis disease, Nausea, Vomiting or Diarrhea, Heart Disease, meningitis, Esquizofrenia, Toxoplasmosis, Pulmonary Fibrosis,Diabetes, Kidney Disease, Lupus, Epilepsy, Stroke,Eczema, Erysipelas Eating Disorder, Back Pain. Osteoporosis etccontact him for your solution.