Burkitt Lymphoma — Causes and Symptoms
Burkitt lymphoma (small non-cleaved cell lymphoma) is one of the most aggressive and rapidly growing non-Hodgkin's lymphomas, with obvious predominance in children and young adults. This type of tumor requires urgent therapeutic intervention as the CNS and the bone marrow are involved in the malignant process since early stages of the disease.
Table of Contents
Are you more of a visual learner? Check out our online video lectures and start your pathology course now for free!
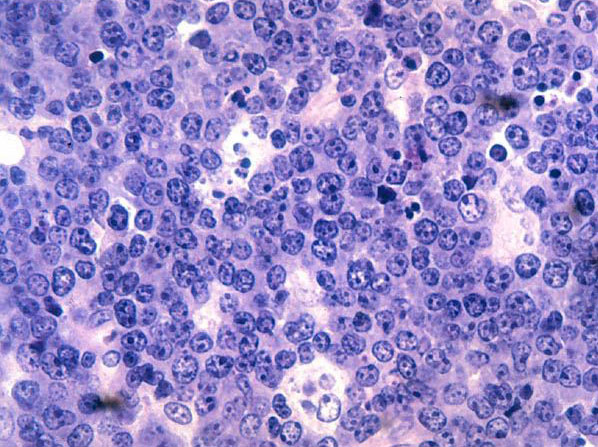
Image: “Malignant B-cell lymphocytes seen in Burkitt’s lymphoma, stained with hematoxylin and eosin (H&E) stain.” License: Public Domain
Definition and Background of Burkitt Lymphoma
Burkitt lymphoma (BL) is an aggressive B-cell non-Hodgkin lymphoma (NHL). It is named after Dr. Denis Burkitt, who described lymphoma in African children (‘African-type’ or ‘endemic’ Burkitt lymphoma). Another type is the ‘sporadic’ or ‘non-endemic’ type that is more common in the Western world.Epidemiology of Burkitt Lymphoma
The incidence of endemic and sporadic Burkitt lymphoma (BL) vary geographically.The endemic BL is found in Africa, hence also called ‘African’ Burkitt lymphoma. The highest incidence of BL occurs in children aged 4-7 years, with an estimated incidence of 4-5 cases per 100,000 children annually. BL accounts for one-third to one-half of all childhood cancers in equatorial Africa. Males are twice more commonly affected than females.
The sporadic or non-endemic BL is common in the United States and Western Europe. It comprises 30% of pediatric lymphomas and less than 1% of adult NHLs in the US, with an estimated incidence of 3 cases per million persons annually. The sporadic BL is also more common in males with an M:F ratio of 3-4:1.
Etiology and Pathophysiology of Burkitt Lymphoma
The cancerogenic process of BL takes place in the germinal centers of the lymphoid organs (Peyer’s patches, spleen and lymph nodes). In BL, a characteristic genetic mutation is observed, i.e., translocation and deregulation of the c-MYC gene (proto-oncogene) on chromosome 8, which is responsible for the development of BL.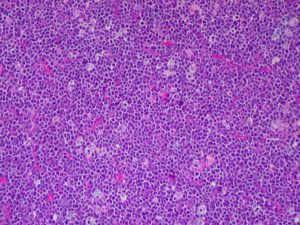
Burkitt lymphoma, by Ed Uthman from Houston, TX, USA, H&EUploaded by CFCF, CC BY 2.0, https://commons.wikimedia.org/w/index.php?curid=30103521
Histologically, BL manifests as a “starry sky” appearance, with the monoclonal proliferation of medium-sized, non-cleaved B-cells that are similar in shape and size; they make up a diffuse pattern of tissue engagement.
Clinical Presentation of Burkitt Lymphoma
The Burkitt lymphoma is a very aggressive B-cell lymphoma that presents with rapidly growing cancer masses that have very short doubling times. The constellation of symptoms of BL depends upon the scale of the lesion, CNS involvement and the effect on contiguous organs.
Picture of the mouth of a patient with Burkitt lymphoma showing disruption of teeth and partial obstruction of the airway,” by Mike Blyth – Own work. License: CC BY-SA 2.5
The sporadic BL often presents with primary abdominal involvement, such as abdominal masses, distension and ascites involving the stomach and intestines. The bone marrow is also involved in about one-third of the cases.
The BL, like other NHLs, is associated with painless lymphadenopathy, which is more common in adults rather than in children. Patients with BL may present with the constitutional symptoms, called B-symptoms, such as fatigue, night sweats, loss of weight. They are often exhausted, complain about vomiting, thirst and dizziness. The condition may also manifest like a severe intoxication with signs of kidney failure. All symptoms are characterized by swift turnover of mature B-lymphocytes.

By Mike Blyth – Own work, CC BY-SA 2.5, https://commons.wikimedia.org/w/index.php?curid=1504829
- Abdominal masses
- Ascites
- Hepatosplenomegaly
- Ecchymosis and/or petechiae (as a result of thrombocytopenia) “dot-like” skin hemorrhage
- Meningeal signs (from CNS disease), confusion, headaches, impairment of eye sight and paraplegia
Laboratory studies
- Excisional biopsy (important for confirmation of diagnosis).
- Complete blood cell (CBC) count with differentials:
- In the case of bone marrow involvement, there is pancytopenia.
- Coagulation tests (prothrombin time [PT], partial thromboplastin time [PTT] and fibrinogen) in order to detect and evaluate the probability of disseminated intravascular coagulopathy (DIC).
- Serum electrolyte levels:
- In BL, there is hyperkalemia, hyperphosphatemia, hyperuricemia and hypocalcemia.
- If uric acid levels are high, this is evidential of high-grade malignancy.
- Lactate dehydrogenase is extremely elevated.
- Creatinine (kidney function tests).
- The abnormal serum electrolytes, a very high serum lactate dehydrogenase (LDH) levels and hyperuricemia may occur due to spontaneous tumor lysis.
- Liver function tests
- Tests for human immunodeficiency virus (HIV) and hepatitis B (HBV) infection for all patients.
- Beta2 microglobulin is a sign of extension of the disease and its relapse.
- Immunophenotype and cytogenetic studies.
Imaging studies
- Head or spinal computed tomography (CT) scanning;
- Magnetic resonance imaging (MRI);
- Bone scanning and plain bone radiography.
Staging of Burkitt Lymphoma
St. Jude/Murphy staging system for Burkitt lymphoma
| Stage I | There is a solitary tumor (extranodal) or single anatomic area (nodal); abdomen and mediastinum are not involved in the process. |
| Stage II |
|
| Stage IIR | Completely resected intra-abdominal disease |
| Stage III |
|
| Stage IIIA | Localized but non-resectable intra-abdominal disease. |
| Stage IIIB | Widespread multiorgan abdominal disease. |
| Stage IV | Any of the above with initial CNS and/or bone marrow involvement (less than 25% involvement; greater than 25% involvement is defined as L3ALL- acute lymphoblastic leukemia). |
Management of Burkitt Lymphoma
The mainstream therapy in the management of Burkitt lymphoma is chemotherapy. The common chemotherapeutic agents used to treat BL include:- CODOX-M/IVAC (Magrath regimen) (cyclophosphamide, vincristine, doxorubicin, high-dose methotrexate / ifosfamide, etoposide, high-dose cytarabine) and the CALGB 9251 protocol-intensive and short-term therapy.
- Hyper-CVAD (modified fractionated cyclophosphamide, vincristine, doxorubicin, dexamethasone) and the Cancer and Leukemia Group B (CALGB) 8811 protocol-long-term therapy.
- Rituximab is added to the mainstream therapy.
- Urate-oxidase enzymes (rasburicase).
- Glucocorticoids (prednisone as the remedy for immunosuppression).
Radiotherapy and surgery are not the recommended options in Burkitt lymphoma.
Supportive Therapy
As the hemopoiesis is oppressed in Burkitt lymphoma, the transfusions of the blood elements are compulsory (red blood cells or platelets) in the case of anemia and thrombocytopenia.Intravenous antibiotics are administered for neutropenic fevers and CNS involvement.
Intravenous fluids are administered to adequately hydrate the patient and maintain high urine output in order to prevent tumor lysis syndrome.



{kind=link}
Comentários
Enviar um comentário