Gallstones — Causes, Risks and Treatment
In Lecturio - Gallstones are common in the United States, especially among the Hispanic population. They are common among the fatty fertile females in their forties. The gallstones are mostly asymptomatic that do not need treatment except in certain high-risk groups. The symptomatic patients present with right upper quadrant abdominal pain and cholecystectomy is the primary treatment option in these patients.
Table of Contents
Are you more of a visual learner? Check out our online video lectures and start your pathology course now for free!

Image: “Opened gall bladder containing numerous gallstones.” by Emmanuelm at en.wikipedia. License: CC BY 3.0
Background
Gallstones are the stones in the gallbladder that are formed when bile fluid becomes hardened inside the gallbladder. The stones can also be as a result of cholesterol or pigment hardening or a combination of both.Biliary colic is the pain in right upper quadrant of the abdomen that results when a gallstone temporarily impacts the cystic duct during a contraction. It is as a result of gallbladder contractions.
Acute cholecystitis occurs when there is a prolonged obstruction of the cystic duct and secondary bacterial infection of the gallbladder resulting in right upper quadrant abdominal pain, fever, and abdominal tenderness.
The majority of gallstones are cholesterol based and are asymptomatic. When symptomatic, the most common presentation is recurrent right-upper-quadrant abdominal pain that is associated with nausea and vomiting and could have a temporal relationship with high-fat content food intake.
The treatment is surgical removal of the gallbladder (cholecystectomy). The current consensus is to treat symptomatic gallstones only. However, in certain populations, a prophylactic cholecystectomy is offered, such as children with sickle cell disease. It is also indicated for spinal injury patients, persons with calcified/nonfunctional gallbladder as well as those whose gallstones have enlarged past two centimeters.
Pathophysiology of Biliary Disease
Bile is formed by the liver and is stored and concentrated in the gallbladder, which contracts after fatty meals to deliver the bile into the intestine. Bile is mainly composed of cholesterol, bile salts, phospholipids and inorganic acids and helps in fat emulsification and absorption in the small intestine.
Precipitation of bile salts and cholesterol gives rise to gallstones. Formation of a nadir of insoluble cholesterol or mucus is the primary step followed by multiple layers of precipitation until the stone is formed. This may be due to either over-concentration of bile, or over-secretion of mucus or bile stasis.
Bile stasis is clinically significant in diabetic patients who have intestinal hypomobility, comatose patients in the ICU or under total parental nutrition, pregnant women and those with oral contraceptive use.
20 % of the population will have biliary complaints and 20 % of patients will have serious complications, ranging from gallstones to pancreatitis and intestinal obstruction.
The size of gallstones plays an important role in the symptomatology of the patient. Larger stones result in the typical right-upper quadrant pain experienced in gallstones, while smaller ones tend to lodge down and block the pancreatic duct causing pancreatitis.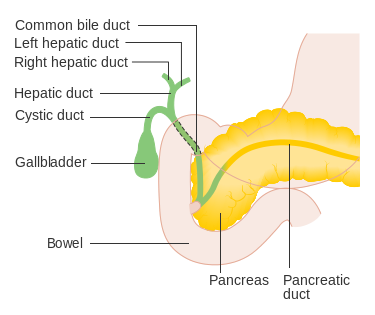
Image: “Diagram Showing the Position of the Bile Ducts.” by Cancer Research UK uploader. License: CC BY-SA 4.0
Epidemiology of Gallstones
While gallstones are found among all age groups, they are more common in Females, who are Fertile, obese (Fatty) and in their Forties (the 4 Fs). In one study, it was estimated that 25 % of women older than 60 years are expected to have gallstones.Despite this high prevalence of gallstones, only 20 % of the patients are symptomatic and approximately 2 % of people are expected to become symptomatic per year. Because of this low risk, asymptomatic patients are not surgically treated.
The prevalence of gallstone increases with age and women are twice as likely to develop gallstones. This is thought to be due to a higher cholesterol blood level that is related to high estrogen states, such as in pregnancy or when on combined oral contraceptives.
People who are at an increased risk of dyslipidemia such as the obese, diabetics, having the sedentary lifestyle and those who attempt to lose weight rapidly, are also all at an increased risk of gallstones.
Additionally, gallstones are more common in certain races, such as Native Americans, Hispanics, followed by North Americans, Europeans and, finally, Asian populations. Finally, certain drugs have been linked to an increased risk of gallstones, such as fibrates and chronic use of proton pump inhibitors.
Around 10,000 deaths are attributed to gallstones in the US annually which arise from gallstone complications, gallbladder cancer and complications in cholecystectomy. On international standards this rate maybe higher due to liver flukes infestations.
Types of gallstones
Cholesterol stones are the most common gallstones. They develop in women more often than in men, with risk factors like obesity, cystic fibrosis, clofibrate, and malabsorption. Estrogen hormone makes women susceptible to gallstones during pregnancy as well as through use of oral contraceptives.- Pure cholesterol stones are solitary, white in color and larger than 2.5 cm.
- Mixed cholesterol stones with 50 % cholesterol are multiple, small and laminated into layers of dark and light pigment stones.
- Black stones are formed of polymerization of calcium bilirubinate inside the gallbladder. The excess bile pigment is common in patients with hemolytic anemia and alcoholic liver disease.
- Brown stones are common inside the ducts from bacterial enzymes that precipitate bile pigment. They can be associated with duodenal diverticula.
Etiologies of cholesterol gallstones
Cholesterol gallstones are formed when bile cholesterol concentration increases. These patients are expected to have excessive cholesterol biosynthesis, the inability to convert cholesterol to bile acids, or an interruption of the enterohepatic circulation.Obese people and patients with genetic predisposition to hyperlipidemia, such as familial hypercholesterolemia have excessive cholesterol biosynthesis. Additionally, diabetics are known to have hypertriglyceridemia, which predisposes them to cholesterol gallstones.
Older age and higher estrogen states have been linked to a decreased cholesterol 7-alpha-hydroxylase enzyme activity, which results in the diminished conversion of cholesterol to bile acid and eventually, cholesterol becomes less soluble in the bile and stones form.
Interruption of the enterohepatic circulation could happen after gastrointestinal surgery or overnight fasting.
Etiologies of pigment gallstones
Pigment gallstones are the result of excessive bilirubin, unlike cholesterol gallstones. Excessive bilirubin is associated with hemolysis, cirrhosis, and infection with beta-glucuronidase producing bacteria. Pigment stones are more likely to be calcified and visible on plain X-ray.
Image: “Photomicrograph of normal-shaped and sickle-shape red blood cells from a patient with sickle cell disease.” by Gregory Kato – Own work. License: CC BY-SA 4.0
- Black pigment stones result from chronic hemolytic diseases, such as thalassemia, sickle cell disease, and hereditary spherocytosis. Cirrhosis can also cause black pigment gallstones.
- Brown pigment stones, on the other hand, are usually the result of beta-glucuronidase bacterial infections of the gallbladder. Beta-glucuronidase hydrolyzes conjugated bilirubin and renders it as unconjugated bilirubin. Unconjugated bilirubin is more likely to form calcium salts, which are not soluble and form gallstones. Brown pigment stones are also more common in Asians populations.
Clinical Presentation of Gallstones
The majority of patients with gallstones are asymptomatic but these patients can have non-related gastrointestinal symptoms such as flatulence, irritable bowel syndrome, postprandial distress, heartburn, bloating, constipation or diarrhea and gallstones are incidentally identified on an ultrasonography.Symptomatic patients, on the other hand, are more likely to present with right-sided upper quadrant abdominal pain that describes a more specific picture of biliary colic. Biliary colic results when a stone temporarily impacts the cystic duct during a contraction. The pain reaches maximum intensity in the right upper quadrant in 20 minutes after the ingestion of a fatty meal and eventually resolves in one to two hours. It is intense and not truly colicky in nature. Less specific symptoms include vomiting, nausea, dyspepsia and fat intolerance.
Physical examination is important in patients with biliary colic to differentiate them from acute cholecystitis cases. Tenderness and rebound tenderness are the markers of gallbladder inflammation that are unlikely in biliary colic where inflammation is not implicated. Fever is also more specific of cholecystitis, rather than biliary colic.
Acute cholecystitis occurs when there is a prolonged obstruction of the cystic duct and secondary bacterial infection of the gallbladder. Chronic gallbladder stones put the patient at an increased risk of gallbladder wall fibrosis and cancer.
Diagnostic Workup of Gallstones Disease
Laboratory investigations can help exclude an acute inflammatory process but are usually unhelpful in simple biliary colic. Abdominal X-rays, ultrasonography, computed tomography, magnetic resonance imaging and nuclear scintigraphy, are all used in the diagnostic workup of patients with gallstones. Auscultation, palpating the abdomen, as well as obesity should also be noted when making diagnosis.Laboratory investigations in gallstones disease
Acute cholecystitis is associated with neutrophils leukocytosis in two-thirds of the patients. Liver enzymes might be slightly impaired in acute cholecystitis. Amylase levels and lipase are also important to exclude acute pancreatitis, especially if the ultrasonography shows small gallbladder stones.Common bile duct stones, another complication of gallstones, result in an increase in alanine and aspartate aminotransferases levels at first and followed by an increase in bilirubin.
Blood tests
The blood test will focus on the blood count, liver function, amylase as well as lipase components.Ultrasonography
Transabdominal ultrasonography is the best imaging modality to diagnose gallbladder stones. It is non-invasive, cheap, sensitive and specific. Gallbladder stones are echogenic on ultrasonography and have an acoustic shadow as seen in the figure.
Image: “Ultrasound Image of Gallbladder Stone.” by © Nevit Dilmen. License: CC BY-SA 3.0
Abdominal plain X-ray
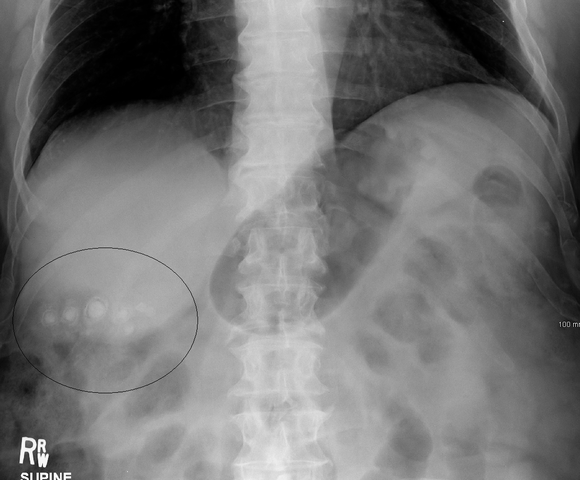
Image: “Gallstones as seen on plain x-ray.” by James Heilman, MD – Own work. License: CC BY-SA 3.0
Abdominal X-rays also help exclude other differential diagnoses, such as renal stones, calcific pancreatitis, and intestinal obstruction.
Computed tomography (CT) scan
CT abdominal scanning is used to exclude other causes of abdominal pain when one is not certain about gallstones as the etiology. It has a low sensitivity for gallstones and is expensive if compared to the more specific and faster ultrasonography scan.Magnetic resonance cholangiopancreatography (MRCP)
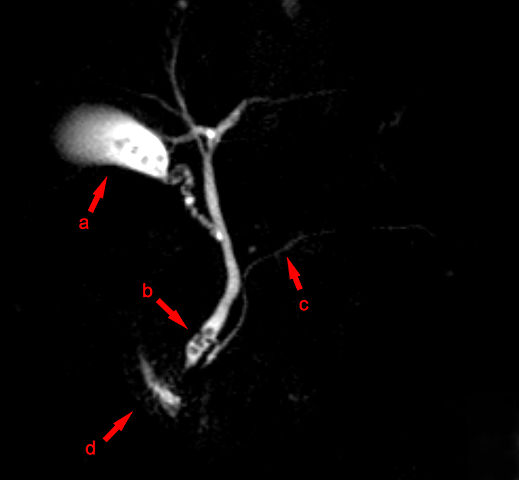
Image: “MRCP: (a) gallbladder with gallstones, (b) stones in the bile duct, (c) pancreatic duct, (d) fluid in duodenum.” by Hellerhoff – Own work. License: CC BY-SA 3.0
Technetium-99m (99m Tc) hepatoiminodiacetic acid (HIDA)
HIDA scintigraphy is only useful in patients with acute cholecystitis with an obstructed cystic duct. A recent meta-analysis showed that patients with a positive HIDA scan result and a negative ultrasonography will always benefit from a cholecystectomy.Endoscopic retrograde cholangiopancreatography (ERCP)
ERCP is often used in patients with common bile duct stones. It is both diagnostic and interventional where the stones can be extracted from the common bile duct.Treatment Options for Gallstones
Asymptomatic gallstones should not be offered medical treatment unless they have mild biliary colic and are in a high-risk group for surgical intervention. Any patient with symptomatic gallstones should be offered a cholecystectomy unless surgery poses a high risk. Medical treatment at the emergency department should mainly include pain control.Treatment of asymptomatic gallstones
People with asymptomatic gallstones should not be offered a surgical intervention. Pregnant women and diabetics are at an increased risk of gallstones disease complications and, if asymptomatic gallstones are identified, it should be followed-up closely.Despite this, certain patients with asymptomatic gallstones should undergo a cholecystectomy. For example, patients with stones larger than 2 cm in diameter, gallbladder wall calcification, patients with spinal cord injuries and, in sickle cell disease, asymptomatic gallstones are indicated for a cholecystectomy.
Ursodeoxycholic acid (ursodiol) can be used to dissolve pure cholesterol stones in asymptomatic patients, or in patients who cannot undergo surgical intervention. Treatment with ursodiol is successful with small stones and should be attemp ted for at least 6 months. Unfortunately, the recurrence rate after the medical dissolution of gallstones is high and is up to 50 %.
Surgical intervention for gallstones
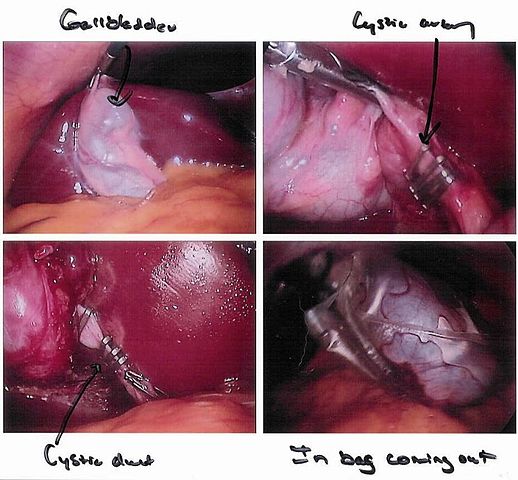
Image: “Pictures of my cholecystectomy in progress taken through the laparoscope.” by User:Pschemp. License: CC BY-SA 3.0
Traditional open cholecystectomy uses a large subcostal incision to remove the gallbladder, which is associated with an increased recovery time and postoperative complications when compared to the modern laparoscopic technique.
Laparoscopic cholecystectomy involves four very small abdominal incisions and can be done in an outpatient setting. If the surgeon cannot catch the escaped gallstones during laparoscopic cholecystectomy, or adhesions and bleeding complications occur, conversion to open cholecystectomy might be required.
Cholecystostomy is indicated in patients with empyema or who are not stable enough to undergo cholecystectomy. Once the patient is stable again, elective cholecystectomy is offered. Cholecystostomy uses a tube that passes through the gallbladder to drain pus.
In a few cases, removal of the common bile duct stones during the surgery is not possible. In this occasion, endoscopic sphincterotomy and ERCP are indicated to extract common bile duct stones. ERCP can also be used in the acutely ill patient and not only in elective cases.
Extracorporeal shockwave lithotripsy
It is effective in pulverizing the stones into smaller fragments that can pass through body painlessly.
Complications of Gallstones
Acute Cholangitis
Cholangitis is the inflammation (infection) of the biliary tree after obstruction irrespective of the cause of obstruction. Charcot triad is very helpful for its diagnosis that consists of fever, right upper quadrant pain, and jaundice. Reynolds pentad of hypotension and altered mental status with the triad is a bad prognostic indicator for severe biliary infection.
Organisms migrating to the biliary tree from the intestine through the portal vein or the biliary tract are responsible for the conditions. E. coli, Pseudomonas, Proteus, Klebsiella and enteric streptococci can be isolated.
Acute pancreatitis
Gallstones are one of the most common causes of acute pancreatitis. It can be due to the obstruction of the pancreatic duct by a stone in the bile duct or backflow of the bile into the pancreatic duct causing activation of pancreatic enzymes resulting in the inflammation of the pancreas.
Porcelain gallbladder
The chronic gallstones irritate the gallbladder wall leading to extensive calcium deposition. This brittle gallbladder with high calcium content is called porcelain gallbladder and has a high association with gallbladder adenocarcinoma. It is often an incidental finding and cholecystectomy is usually performed due to a higher risk of cancer.Mirizzi syndrome
Impaction of a gallbladder stone in the cystic duct can cause external compression and subsequent obstruction of either the common bile duct or the hepatic duct. Obstruction of both ducts can result in necrosis of the wall, fistula or scar formation and obstructive jaundice will develop. Chronis obstruction in the cystic duct, as well as gallbladder tumor, may develop in the right upper abdomen in a patient without jaundice if there is formation of palpable mass.
Gallbladder Hydrops
It is due to blockage of gallbladder or mucosal inflammation which results to the gallbladder distending due to mucoid fluid that is clear and uninfected. It requires cholecystectomy but if it is related to Kawasaki disease it usually resolves itself.
Conclusion
Gallstones are common in fatty fertile females in their forties (4-Fs). While the majority of the cases are asymptomatic, only 2 % of asymptomatic gallstones are expected to become symptomatic per year.Asymptomatic gallstones should not be treated except for certain populations that are known to be at high risk for the development of symptomatic disease and complications, while symptomatic patients should undergo a cholecystectomy. Laparoscopic cholecystectomy is superior to open cholecystectomy but, in a few cases, the surgeon might need to convert to an open procedure.
Finally, patients with symptomatic gallstones, who are not possible candidates for surgical intervention, should be prescribed a gallstone dissolution agent if the stones are expected to be purely made of cholesterol



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comentários
Enviar um comentário