Anorexia, Bulimia, Binge-Eating: An Overview of Eating Disorders
Table of Contents
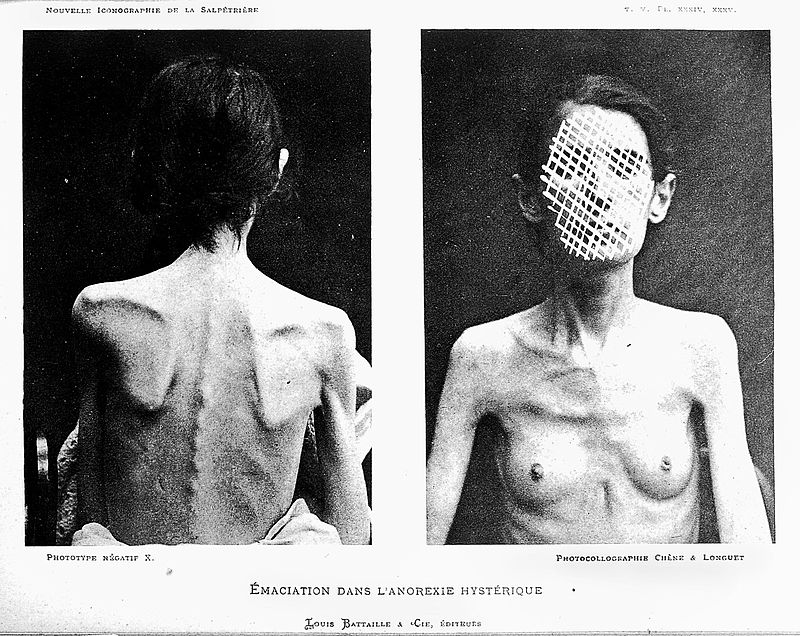
Picture: “Anorexic emaciation in a hysteric General Collections Keywords: Psychiatry” by Welcome Images. License: CC BY 4.0
Definitions of Eating Disorders
Eating disorder: It is a chronic psychiatric condition characterized by a persistent disturbance of eating behavior that has a significant negative impact on physical health and/or psychosocial functioning.
Anorexia nervosa: It is an eating disorder characterized by self-imposed starvation and inappropriate dietary habits, due to a morbid fear of weight gain and disturbed perception of body shape and weight. These patients are often emaciated and their body weight often drops below 85 % of ideal body weight with associated physiologic and psychologic complications.
Bulimia nervosa: It is an eating disorder characterized by recurrent episodes of binge eatingaccompanied by inappropriate compensatory behavior to counteract the effect of binge eating.
Binge eating disorder: It is an eating disorder characterized by recurrent episodes of binge eating without inappropriate compensatory behavior.
Epidemiology of Eating Disorders
The eating disorders have a higher prevalence in the younger population, mostly affecting the female gender, and are far more frequent in higher social classes and in the developed countries.
Anorexia nervosa is common in young females of ages 15 to 25 years and has a prevalence of about 1 %. The ballet dancers, athletes, and models are the most frequently affected.
Bulimia nervosa has a prevalence of 2—4 % of the young adult population. The females of ages 18 to 35 are most commonly affected.
Binge eating disorder has a prevalence of 2—5 % throughout the population. About one-half patients affected are overweight, and one-third of all cases are males.
Etiology of Eating Disorders
The etiology of all eating disorders cannot be tracked back to a single event, but consist of a complex interaction between biological, psychological and social factors. Studies of twins show that genetic factors also play a role in their pathogenesis.
All eating disorders have in common a disturbed perception of body shape and weight. To avoid weight gain and to reduce weight, people use measures like fasting, physical strain, and laxatives, which more usually than not result in organic consequential diseases.
These patients often have a disturbed self-image and self-esteem, and they also have a higher prevalence of other disorders such as obsessive-compulsive disorders, affective disorders or impulse-control disorders.
Anorexia Nervosa
“Anorexia” literally means “loss of appetite,” which, strictly speaking, does not apply to this disease. The patients experience hunger sensations but deny them and try to suppress them due to fear of gaining weight.
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-V) defines the following criteria for the diagnosis of anorexia nervosa:
- Restricted dietary habits resulting in significantly low body weight.
- Intense fear of gain weight.
- Perceived disturbance in body weight and shape.
Classification of Anorexia Nervosa
Anorexia nervosa is classified into the following two types depending upon the dietary behavior:
- Restrictive type: characterized by excessive starvation.
- Purging type: characterized by the use of drugs (laxatives, diuretics), induced vomiting, and excessive exercise as a mean to reduce weight.
Clinical Features of anorexia nervosa
The characteristic symptoms of anorexia nervosa are the excessive fear of weight gain, along with a body image disturbance. They consider themselves too fat despite being underweight and often find their own body displeasing. These symptoms hamper their daily activities and they are preoccupied with the weight issues. Additionally, these patients lack disease awareness, therefore, the compliance is very little or absent, especially at the beginning of treatment.
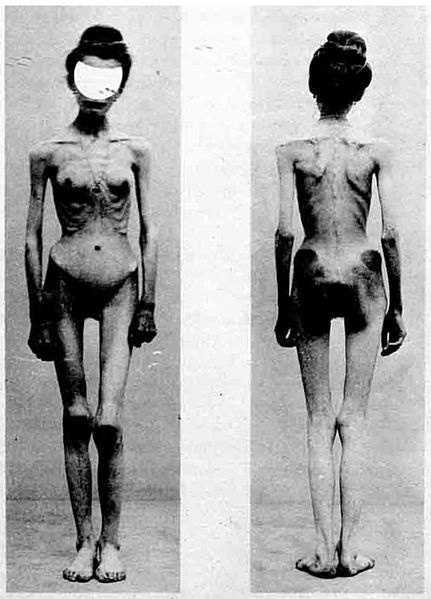
Picture: “Two images of an anorexic female patient in the French medical journal Nouvelle Iconographie de la Salpêtrière vol 13, published in 1900,” by Georges Gasne. License: Public Domain
On systemic review, the patients may additionally have the following symptoms:
- Difficulty in concentration and decision-making
- Mental health concerns (for example, anxiety, depression, social withdrawal)
- Amenorrhea
- Headaches
- Dizziness
- Lethargy
On physical examination, the patients are markedly underweight and have a body mass index (BMI) of less than 17.5 kg/m2. The following additional signs may be present on the examination:
- Hypotension
- Bradycardia
- Hypothermia
- Dry skin
- Lanugo body hair/Thin hair
- Breasts atrophy
- Swelling of the salivary glands
- Peripheral edema
Treatment of anorexia
The treatment of anorexia nervosa consists of a combination of psychotherapy and pharmacotherapy.
Anorexia nervosa has widespread effects on all the body systems and can be life-threatening. In most cases, hospitalization is advisable to get the patients out of the environment which promotes the disorder. During the hospital stay, the goal of therapy is to gain approximately 0.5 to 1 kg of weight per week. Initially, force-feeding with parenteral electrolyte solutions and a nasoduodenal tube may be necessary. The electrolytes are regularly checked as refeeding syndrome may occur.
The refeeding syndrome is a constellation of metabolic disturbances that occur due to refeeding of malnourished patients who are persistently starved, as in the case of anorexia nervosa. It occurs due to sudden shifting of fluid and electrolytes resulting in marked electrolyte disturbances (with the hallmark feature being hypophosphatemia), seizures, delirium, and can be fatal.
In depressive patients, short-term application of antidepressants or neuroleptics can be reasonable. Due to the low disease awareness of the patients, therapy often is very difficult and spans over a period of several months to years.
Bulimia Nervosa
The DSM-V defines the following criteria for the diagnosis of bulimia nervosa:
- Recurrent episodic binge-eating.
- Recurrent inappropriate compensatory behaviors to prevent weight gains, such as fasting, the use of laxatives and diuretics, self-induced vomiting, fasting, or excessive exercise.
- Excessive emphasis on body shape or weight.
Clinical Features of Bulimia Nervosa
The characteristic symptoms of patients with bulimia nervosa are recurring ravenous hunger attacks accompanied by the intake of large amounts of high-calorie foods. Following these binge-eating episodes, there arise feelings of guilt and shame that result in the counter-regulatory measures (self-induced vomiting, laxatives, diuretics, fasting, excessive exercise and thyroid gland preparation) to avoid the effects of gaining weight.
In contrast to anorexics, bulimic patients mostly are of normal weight (sometimes slightly overweight) and it is sometimes the only differentiating point between them. They do not suffer from a body image disorder; however, they exhibit high psychological strain. They are often conscious of their disturbed eating behavior and are ashamed of it, and use methods to hide it.
More than two-thirds of the patients show psychological comorbidities, e.g., depression, anxiety, and suicidal inclinations.
The physical examination may include the following signs:
- Dental caries caused by repetitive self-induced vomiting.
- Swollen parotid glands.
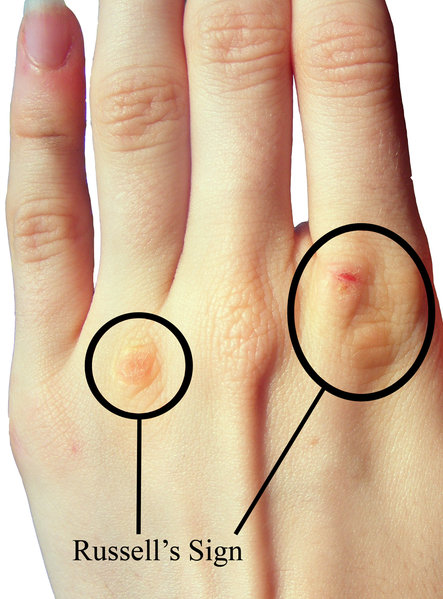
- Due to self-afflicted vomiting, lesions on the back of the hand can be found in some cases (“Russell’s sign”).
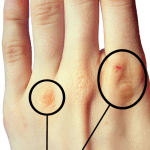
- Picture: “Russell’s Sign on the knuckles of the index and ring fingers.” by Kyukyusha. License: Public Domain

- Picture: “Oral Manifestation of Bulimia.” by Jeffrey Dorfman. License: CC BY-SA 3.0

Treatment of bulimia
Like anorexia nervosa, the treatment of bulimia consists of a combination of psychotherapy and pharmacotherapy.
Psychotherapy—and more precisely, cognitive behavioral therapy is the first resort therapy. The goal is to normalize the patient’s eating behavior and avoid the destructive binge eating attacks. Furthermore, their self-esteem has to be strengthened, while the fear of gaining weight has to be decreased.
Concerning pharmacotherapy, tricyclic antidepressants, selective reuptake inhibitors (e.g., fluoxetine) are suitable, while monoaminoxidase inhibitors are useful for treating depressive coexisting symptoms and relapse prophylaxis.
Should ambulant therapy fail, or in the case of self-injuring behavior or increased risk of suicidal tendencies, hospitalization may be necessary.
Binge Eating Disorder
The DSM-V defines the following criteria for the diagnosis of binge-eating disorder:
- Recurrent episodes of binge eating.
- Marked distress regarding binge eating.
- Absence of inappropriate compensatory behavior (unlike bulimia nervosa).
Clinical Features of Binge Eating Disorder
The characteristic symptoms of patients with binge eating disorder are recurring cravings accompanied by the intake of large amounts of high-calorie foods. Following these binge-eating episodes, there arise feelings of guilt and shame but the counter-regulatory measures are absent following the binge eating episodes (unlike bulimia).
In contrast to anorexia and bulimia, the patients are mostly overweight or obese. One-third of all cases are men.
Treatment of Binge Eating Disorder
It is important to treat not only the patients’ dietary symptoms but also the underlying psychiatric issues (depression, anxiety, low self-esteem) and comorbidities (obesity, hypertension etc).
Similar to the other eating disorders, treatment is attempted with the combination of psychotherapy via cognitive behavior therapy, and medications (SSRI, TCA etc).
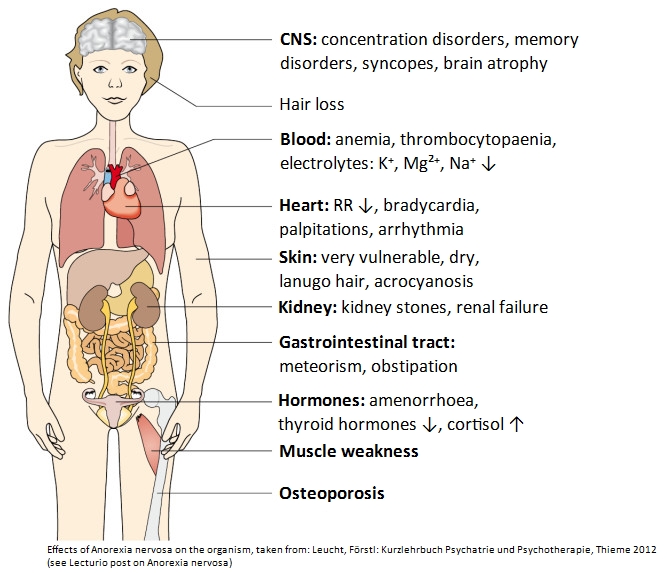
Symptoms of Eating Disorders in an Overview
Review Questions
The correct answers can be found below the references.
1. Bulimia nervosa mostly occurs in women between the ages of 18 to 35 years. Which symptom is not typical for this disease?
- The high psychological strain of the patients.
- Feeling of control loss.
- Shame and feelings of guilt due to the disturbed eating behavior.
- Bad compliance in the therapy of the disease.
- Repeated episodes of eating attacks with subsequent counter-regulatory measures.
2. A 17-year-old girl visits her family doctor due to concentration problems and decreased performance. On physical examination, she has a height of 1.60 m and weighs 44 kg. Upon inquiry, however, the patient, states that she feels well except for decreased performance. She experiences her physical state as normal. Furthermore, she requests her doctor to help her quickly become productive in school again. Which disease matches her symptoms?
- Binge eating disorder
- Anorexia nervosa
- Diabetes mellitus
- Hypothyroidism
- Bulimia nervosa
3. Anorexia is often accompanied by organic consequential diseases. Which of the following symptoms does not apply to anorexia nervosa?
- Alopecia
- Amenorrhea
- Hypokalemia
- Osteoporosis
- Decreased cortisol levels



{kind=link}
Comentários
Enviar um comentário