Testicular Torsion — Diagnosis and Treatment
Table of Contents
- Definition of Testicular Torsion
- Epidemiology of Testicular Torsion
- Pathophysiology of Testicular Torsion
- Clinical Presentation of Testicular Torsion
- Diagnostic Work-up for Testicular Torsion
- Treatment of Testicular Torsion
- Complications of Testicular Torsion
- Prognosis of Testicular Torsion
- References
Image : “Check your #testicles after a shower or bath is the best time to check them @ballstocancer” by GioBertPhoto
. License: CC BY-SA 2.0
Definition of Testicular Torsion
Testicular torsion is a medical emergency in which the spermatic cord along with the spermatic artery inside it undergo torsion. Torsion of the spermatic cord results in impaired blood flow to the ipsilateral testis and if left untreated results in testicular necrosis and subsequent infertility.
Testicular torsion can be either intravaginal or extravaginal depending on whether the cord is twisted inside the tunica vaginalis or not.
Epidemiology of Testicular Torsion
Intravaginal torsion is a common cause of acute scrotal pain and is defined as the cause of emergency scrotal pain in approximately 16% of the patients. Intravaginal torsion is more common in adolescents but has been described in patients younger than 30 years of age.
Extravaginal torsion occurs in neonates and is responsible for 5% of all torsions. It is associated with a high birth weight and is usually unilateral. Extravaginal torsion happens prenatally in the majority of the cases.
Bilateral testicular torsion is rare and has been reported in approximately 2% of the cases.
The current incidence of testicular torsion in men younger than 25 years of age is estimated to be 1 in 4,000.
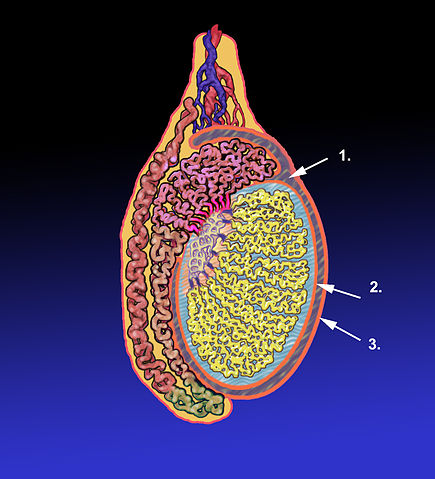
Image: “Diagram of an adult human testicle with the tunica vaginalis pointed out.” by KDS444 – Own work. License: CC BY-SA 3.0
The etiology of testicular torsion is different depending on whether it is extravaginal or intravaginal. In neonates, the spermatic cord is still mobile because it is not fixated yet to the tunica vaginalis. Accordingly, the spermatic cord is free to move and can twist around itself, impairing blood supply to the testis. This can happen prenatally or postnatally.
Intravaginal testicular torsion is common in men with poorly fixated spermatic cords where the tunica vaginalis is too high or partly mobile. This results in a mobile spermatic cord that can also twist around itself in the tunica vaginalis. This congenital abnormality is usually bilateral; hence, bilateral fixation of the testesis indicated in patients with unilateral testicular torsion.
Pathophysiology of Testicular Torsion
In neonates, the testis is still not in the scrotum as it is still descending. This means that the testis is still mobile and is not fixated to the tunica vaginalis. The testis can undergo torsion and this will twist the spermatic cord and kink the spermatic artery. The consequence would be impaired blood supply to the testis and testicular torsion.
In some men, the tunica vaginalis is abnormally attached and the spermatic cord is not adequately fixated. Again, this results in a mobile spermatic cord that can twist and predisposes the patient to testicular torsion.
Abnormal high attachment of the tunica vaginalis is common and is encountered in approximately 12% of men and is bilateral in 40% of the cases. Because of this, patients with unilateral testicular torsion should undergo bilateral testicular fixation surgery.
Testicular torsion results in impaired arterial blood supply and venous drainage. Eventually, the testis undergoes infarction. The testis can still be viable after approximately 8 hours of torsion, but if testicular torsion is untreated for more than 24 hours the chances are that the testis has already become necrotic and is no longer viable.
Clinical Presentation of Testicular Torsion
Patients with intravaginal testicular torsion present with sudden severe unilateral scrotal pain and swelling. Patients might describe a recent strenuous exercise or trauma to the testis.
Patients also can have nausea, vomiting and the pain is usually of less than 6 hours of duration. Patients with more gradual onset pain are more likely to have epididymitis rather than testicular torsion.
On physical examination, the testis is usually very tender to touch. Scrotal redness is also common. When the pain is not too severe, elevation of the testis can relieve pain in epididymitis but not in testicular torsion but again this is usually difficult to do in patients with testicular torsion because the testis is extremely tender to touch.
Diagnostic Work-up for Testicular Torsion
Once the diagnosis of testicular torsion is suspected from clinical examination and history, emergency surgery to salvage the testis is indicated and no further workup should be performed.
When the pain is gradual, recurrent or severe, imaging studies can be performed. Color Doppler studies can be used to evaluate the arterial blood flow to the testis. In testicular torsion, there is decreased blood flow to the testicle, and this is usually enough to go for surgery.
While Doppler ultrasonography is unlikely to result in false-negative results, it can have a significant number of false-positives. Still, surgery benefits clearly outweigh the risks and any patient with suspected testicular torsion should always undergo an exploratory surgery.
Treatment of Testicular Torsion
Treatment of testicular torsion is surgical. The main goals of surgical treatment are to do testicular detorsion, to save the testis from further necrosis and to preserve fertility. If treatment is delayed, orchiectomy is indicated.
During surgery, the testis should undergo detorsion. Once this is performed, the testis should go back to normal color and a Doppler study should reveal return of normal blood flow to the testis.
If the testis is no longer viable, it should be removed to avoid complications such as testicular infection. After detorsion, the testis should be fixated to the tunica vaginalis to avoid recurrent testicular torsion or detorsion syndrome.
It is always advisable to perform bilateral testicular fixation because the tunica vaginalis is abnormally attached in approximately 40% of the cases bilaterally.
If the testis is not viable, it should be removed and a testicular prosthesis can be implanted for cosmetic reasons. Implantation of the testicular prosthesis should be performed six months after the orchiectomy to allow time for scrotal healing and for the inflammatory process to subside.
Complications of Testicular Torsion
Complications include:
- Loss of testes
- Infection of testes
- Infarction of testes
- Infertility
- Cosmetic disfigurement
- Testicular exocrine and endocrine functions are disturbed. Quality of semen is also affected.
Prognosis of Testicular Torsion
Prognosis depends upon the immediate testicular restoration and onset of testicular atrophy.
Testicular restoration further is determined by the time elapsed between the onset of torsion and initiation of management.Chances of testicular preservation can be as follows:
- < 6 hours: 90—100 %
- 12—24 hours: 20—50 %
- > 24 hours: 0—10 %



{kind=link}
It was my last hope of having a child and Dr Obodo made my dreams come true. I asked for the spells, but didn’t tell my husband. We carried on trying to get pregnant as normal. I had a really good feeling about Obodo. I felt pregnant or like pregnancy was coming very about a week after the spells were cast. I began to vomit in the morning from morning sickness. I thought it was the toast. I’ve never felt like that before. And it was true! I went and grabbed the pee stick to show my husband. I went to my doctors at the earliest possible time to have a test and it came back positive. I immediately rang up my husband to let him know that the pee stick was not a false positive. He asked me how it was possible. He was certain that the pee stick was passed the expiry date. I told him all about Obodo, the fertility spells and he was amazed. We now have a very beautiful baby boy on the way and we are expecting to use Obodo in hope that I can have my baby girl. you can get in touch with doc via info ___ templeofanswer@hotmail . co . uk , call 234 8155 425481 for help
ResponderEliminarThank you,
The Messer Family