Rotator Cuff Tear — Surgical Treatment
Table of Contents
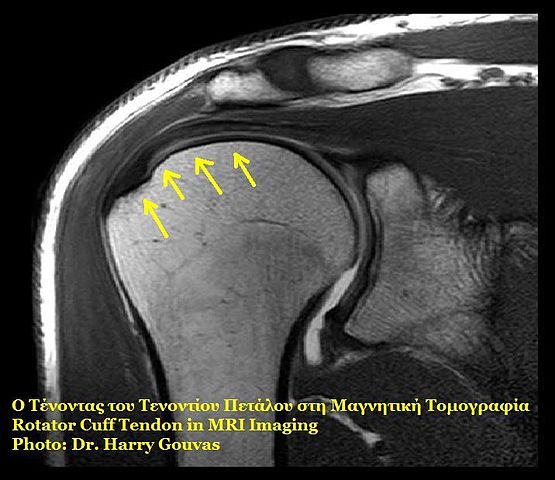
Image: “Rotator cuff.” by Harrygouvas. License: Attribution
Overview of Rotator Cuff Injuries
The rotator cuff refers to a group of muscles and tendons that surround the shoulder joint and perform the various functions of the joint. They include:
- Supraspinatus
- Infraspinatus
- Teres minor
- Subscapularis muscle
Rotator cuff injuries are a spectrum of the same disease process that includes acute reversible tendinitis, chronic tendinitis, and sometimes massive tears of the muscles forming the rotator cuff.
Rotator cuff tears in young adults are usually preceded by a recent history of trauma or repetitive overhead activities. Older adults typically present with non-specific symptoms such as gradual onset progressive shoulder pain; therefore, the diagnosis of rotator cuff injuries in the elderly is usually a radiographic one.
Epidemiology of Rotator Cuff Injuries
Rotator cuff injuries are quite common in the elderly with an estimated prevalence of 40%. This figure only represents patients with complete full-thickness rotator cuff tears. The prevalence of partial rotator cuff tears in the elderly is expected to be even higher than this but, because of the mild symptoms of partial injuries, they are seldom recognized.
One sport that has been extensively studied and connected with the pathophysiology of rotator cuff injuries in the younger adults is baseball. During the late cocking stage and the follow-through of the baseball pitch stage, the rotator cuff muscles are very active. Participating in sports that are characterized by overhead motion mechanisms of the shoulder is the most recognizable risk factor for rotator cuff tears in young adults.
Occupational risk is seen among people who carry out repeated overhead activities such as painters and carpenters.
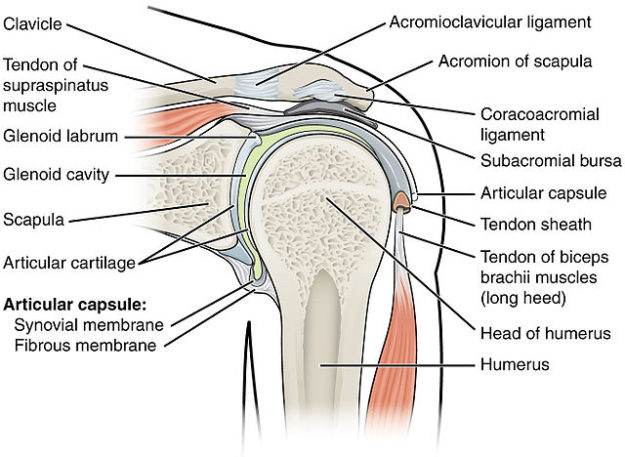
Anatomy of the Shoulder
The shoulder has many joints that include the:
- Sternoclavicular joint,
- Glenohumeral joint (GH), and
- The scapulothoracic joint (ST).
Most of the shoulder range of motion is attributed to the GH and the ST joints.
GH joint
The GH joint is known as a ball-in-socket joint. The glenoid fossa of the scapula is quite flat, and the humeral head is quite big for such a small fossa; therefore, for the humeral head to remain in position, which is required for optimum range of motion, shoulder stabilizers are needed.
Shoulder stabilizers are either dynamic or static. The static stabilizers do not depend on the neuromuscular status of the muscles around the joint. They include the labrum, GH ligaments, and the joint capsule. The three main GH ligaments are found to connect the humeral head to the glenoid anteriorly, inferiorly and posteriorly.
The dynamic stabilizers of the GH joint consist of the rotator cuff muscles and the scapular stabilizers. The rotator cuff muscles include the:
- Supraspinatus,
- Infraspinatus,
- Subscapularis and
- Teres minor.
The main goal of these muscles is to provide stability to the GH joint. The scapular stabiliers are the:
- Teres major,
- Rhomboids,
- Serratus anterior,
- Trapezius, and
- Levator scapula.
Because of their vital role in providing stability to the GH joint, overusing the GH joint, which happens in overhead sports, can cause a shearing force injury of the rotator cuff muscles.
Clinical Presentation of Rotator Cuff Injuries
Goals
The two most important goals of obtaining a clinical history in a patient suspected to have a rotator cuff injury are to confirm the diagnosis and to exclude other differential diagnoses of more life-threatening nature such as cardiac disease. The main complaint of the patient can be any of the following four chief complaints of rotator cuff injuries: limited range of motion, instability, pain or weakness.
An important part of the history is to try to understand if there has been a precipitating risk factor for a rotator cuff injury. A history of overhead sports or a direct shoulder trauma should be excluded.
When the joint’s stability is markedly affected, the patient might complain of numbness, or catching and popping sensations of the humeral head.
Chronic rotator cuff injuries
Patients with chronic rotator cuff injuries typically come after trying different over-the-counter approaches and medications to manage the pain. They may include cold or warm compressors, aspirin, acetaminophen, or non-steroidal anti-inflammatory drugs.
The pain of a rotator cuff injury is usually felt over the anterolateral part of the shoulder.
Overhead activities typically exacerbate the pain. Pain is also more severe at night. Sleeping on the injured shoulder at night might explain the aggravation of pain during the night.
Complete physical examination of the shoulder
Once you have enough clues that the cause of shoulder pain in the patient is shoulder-related and not caused by any other pathology such as ischemic heart disease, you can proceed to perform a complete physical examination of the shoulder. Complete exposure of the shoulder is essential before you start your systematic shoulder examination.
A complete systematic shoulder examination consists of:
- Inspection,
- Palpation,
- Range of motion testing, and
- Motor strength testing.
Inspection of the Shoulder
You should inspect the shoulder from the three main surfaces, anterior, lateral and posterior. You should look for swelling, atrophy, or a small bulge. Remember to always compare with the other shoulder.
Scapular winging is not a common finding in rotator cuff tears. Supraspinatus and infraspinatus atrophy are commonly seen in patients with chronic and complete rotator cuff tears.
Palpation of the Shoulder
Localized tenderness of the greater tuberosity of the humerus is a common finding. The biceps tendon can be also tender due to inflammation.
Range of Motion Testing
Active range of motion in a patient with a rotator cuff tear is usually limited and painful. The ST joint is typically overused during active abduction of the arm compared with a healthy subject. On the other hand, passive range of motion is expected to be normal and intact in a patient with a rotator cuff injury. Significant pain with arm elevation between 60–120 degrees is suggestive of rotator cuff tendons impingement.
Motor Strength Testing
The lift-off test, where the patient is instructed to move the hand away from the back while the arm is internally rotated against resistance, is good to test the motor strength of the subscapularis.
The infraspinatus and teres minor muscles are best examined with the arm and forearm both flexed at 90 degrees and the upper limb is externally rotated.
The supraspinatus muscle is best tested with the passive abduction of both upper arms to more than 90 degrees. The patient is instructed to lower the arms slowly and you should look for a sudden drop of one arm, i.e., the affected side. A positive drop-arm test is indicative of a major rotator cuff tear, especially the supraspinatus.
Diagnostic Workup of Rotator Cuff Injuries
Radiography
Plain radiography is the first diagnostic imaging modality to perform in a patient with a suspected rotator cuff injury. Usually, three views are ordered. The anteroposterior view is optimum for viewing the acromiohumeral distance, which is usually shortened in a patient with a rotator cuff injury. Acromion sclerosis, cystic formation and spurring are suggestive of chronic rotator cuff tendonitis.
The supraspinatus outlet view is used to evaluate the acromion shape and slope. Finally, the axially view is used to study the position of the humeral head to the glenoid fossa.
MRI
Because the rotator cuff includes muscles and their tendons, it is best visualized with magnetic resonance imaging. Magnetic resonance imaging is very specific and sensitive for rotator cuff injuries. This imaging modality can provide information about the location, size, and type of pathology of the rotator cuff.
Ultrasonography
Patients who are unable to perform a magnetic resonance imaging study of the rotator cuff due to cost issues, intolerable pain, or a contraindication to magnetic resonance imaging, might benefit from an ultrasonography. Ultrasonography is very accurate in detecting complete rotator cuff tears. The main disadvantage of ultrasonography over magnetic resonance imaging is the fact that it is highly operator dependent.
Management of Rotator Cuff Injuries
Rest, icing for 20 minutes three to four times a day, and analgesia are the three mainstay treatments for the acute phase of a rotator cuff injury. Analgesia can be either acetaminophen or a non-steroidal anti-inflammatory drug.
Physical Therapy
Once the pain is tolerable and well-managed, the patient is said to have entered the recovery phase. During this phase, the management plan should aim to restore the normal active range of motion of the shoulder, and normalize the strength and stability of the joint.
Physiotherapy combined with some shoulder-specific exercises such as wall walking, or Codman pendulum exercises are usually sufficient to provide excellent results. Strengthening exercises should be limited to the pain-free range of motion only; therefore, the patient should not undergo any extensive strengthening exercise while he or she is in severe pain.
Surgical Intervention
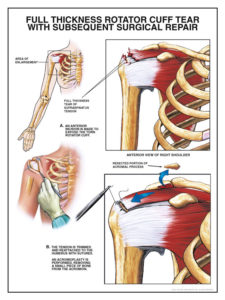
Image: “Rotator cuff high” by Nucleus Communications. License: Attribution
Patients who do not improve within 3–6 months of rehabilitation therapy should receive a surgical intervention. Acromioplasty is a common option here. Patients who receive surgical intervention typically show significant improvement within the first three weeks post-op.
If surgical intervention is being considered, it should be performed as early as possible to prevent fatty degeneration of the rotator cuff teared muscles. Patients with massive rotator cuff injuries might need a tendon replacement surgery.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comentários
Enviar um comentário