Esophageal Diseases: Achalasia, Hiatal Hernia, Diverticulum, GERD, Esophagitis and more
Table of Contents
Image: “Eosinophilic oesophagitis, histologic features” by Mattopaedia. License: CC BY-SA 3.0
Congenital Malformations of the Esophagus
Atresia of esophagus with tracheo-esophageal fistula
Esophageal atresia is a malformation of the esophagus. In the embryonic period, the esophagus develops from the foregut. At first, there is a connection between the airways and the gastrointestinal tract, which is, however, sealed in the course of development by the tracheoesophageal septum, except for the proximal part.
Disorders in this development often lead to a blind-ended superior part of the esophagus and a tracheoesophageal fistula in the inferior part.
An intrauterine complication, which can end in premature labor and premature birth, is the polyhydramnion. The fetus swallows amniotic fluid, which does not reach the gastrointestinal tract due to the malformation and can therefore not be absorbed but rather accumulates. Conspicuous symptoms in a newborn are frequent coughing attacks and salivate, triggered by mislead food and rattling respiration with respiratory disorders, inlcuding even cyanosis.
The disease is often associated with other malformations, the so-called VACTERL association:
- Vertebral malformations
- Anal atresia
- Cardiac malformations
- TracheoEsophageal fistula
- Renal malformations
- Malformations of the Limbs
Functional Disorders of the Esophagus
Achalasia
With an incidence of 1/100,000 inhabitants, achalasia is a rather rare disease with an unknown cause. Even more rarely, it presents in the context of the autosomal recessive triple-A syndrome.
It is characterized by decreased peristalsis of the esophagus and insufficient relaxation of the inferior esophageal sphincter, which leads to the cardinal symptoms dysphagia and retrosternal pain.
Especially when lying down, regurgitation of food accompanied by bad breath occurs, which harbors the potential complications of aspiration pneumonia and esophagitis. This inflammation of the esophagus, referred to as retention esophagitis, increases the risk for carcinoma by 30 times compared to the normal population.
The cause of achalasia is degeneration of the ganglion cells of the myenteric plexus in the inferior part of the esophagus — it is thus neuromuscular. There is a primary form with an unclear genesis as distinguished from a secondary form, which mostly develops in the context of a malignant disease via infiltration of nervous structures.
Diagnosis of achalasia
- Endoscopy with biopsy
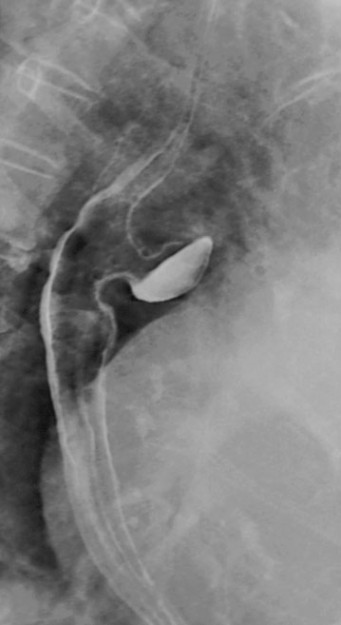
- Barium swallow — which typically shows the so-called “bird’s beak” narrowing with prestenotic dilation (megaesophagus)
- Manometry (physical pressure measurement)

Therapy of achalasia
- Balloon catheter dilation of the inferior esophageal sphincter
- Reversible paresis of the inferior esophageal sphincter with an injection of botulinum toxin
- Surgical cardiomyotomy with the possible complication of post-surgical reflux disease
Esophageal spasm
The esophageal spasm is a rare, benign functional disorder of the esophagus. Retrosternal pain and difficulty swallowing occur in paroxysms and can lead to bolus impaction. In milder cases, glycerol trinitrate is administered. In severe cases, botulinum toxin is injected or surgical interventions are performed.
Hiatal Hernia
In a hiatal/diaphragmatic hernia, the area of the esophageal hiatus of the diaphragm is the hernial orifice through which parts of the stomach or the whole stomach enter into the intrathoracic cavity in the peritoneal hernial sac.
Different forms of the hiatal hernia
Sliding (axial) hernias represent about 90 % of the cases and significantly increase in frequency with age: 50 % of all patients over 50 years old have a sliding hernia. Cardia and fundus of the stomach relocate into the thoracic room. It clinically manifests as reflux disease. In rare cases, bolus obstruction can occur if the superior edge of the hernia has narrowed to form a so-called Schatzki ring.
In a paraesophageal hernia, a part of the stomach—in the most severe case, even the whole stomach (= upside-down stomach)—slides through the hernial orifice beside the esophagus. Paraesophageal hernias can be asymptomatic or show unspecific symptoms, such as belching and pressure in the cardiac area. However, they always carry the risk of incarceration, erosions, ulcers, and bleedings, which is why they are already operated on in the symptom-free stage.
With a share of 5 % of all cases, the mixed hernia as a combination of the sliding hernia and the paraesophageal hernia is rather rare.
Diagnostic of the hiatal hernia
- Barium swallow
- Endoscopy

Image: “Hiatushernie im seitlichen Röntgenbild des Thorax. Pfeil auf Luft-Flüssigkeits-Spiegel.” by Hellerhoff. License: CC BY-SA 3.0
Treatment of hiatal hernia
In cases with a pre-existing reflux disease, sliding hernias are treated symptomatically. Because of the risk of incarceration, paraesophageal hernias are an indication for surgery. In the surgery, the stomach is repositioned and fixed to the anterior abdominal wall, which is referred to as transabdominal gastropexy.
Esophageal Diverticulum
Esophageal diverticula are protrusions in the walls of the esophagus. Small diverticula are often without any symptoms, whereas greater ones mostly cause complaints. Dysphagia, globus sensation, and nocturnal regurgitation of undigested food rests with the risk of aspiration can occur.
The deposition of food residue in these protrusions leads to malodorous fetor ex ore. Diverticula can inflame and form fistulas.
Pulsion diverticula as esophageal diverticula
Pulsion diverticula are considered pseudodiverticula since only mucosa and submucosa are pushed outward through the muscular layers. Predilection sites are the following weak spots in the esophageal muscles:
 Bild: “Pulsionsdivertikel des mittleren Ösophagus.” von Hellerhoff. Lizenz: CC BY-SA 3.0Area of Laimer’s triangle (= an area free of longitudinal muscles at the superior esophagus)
Bild: “Pulsionsdivertikel des mittleren Ösophagus.” von Hellerhoff. Lizenz: CC BY-SA 3.0Area of Laimer’s triangle (= an area free of longitudinal muscles at the superior esophagus)- Above the diaphragm as epiphrenic diverticula (since they are often asymptomatic, they most likely are found as additional findings in x-ray examinations)
Traction diverticula as esophageal diverticula
Traction diverticula are true diverticula since all wall layers are affected by the protrusion (e.g., parabronchial diverticula). They form due to pulling forces from the outside, due to inflammations and processes in the surrounding area of the esophagus.
Diagnosis of traction diverticula
- Barium swallow
- Endoscopy
Treatment of traction diverticula
Clinically relevant cases are treated surgically: diverticula resection.
GERD = Gastro-Esophageal Reflux Disease
While a slight temporary reflux from the stomach into the esophagus is physiological, an increased gastro-esophageal reflux of stomach contents can lead to the gastro-esophageal reflux disease (= GERD). Most patients are severely impaired in terms of life quality. Two forms of GERD can be distinguished:
- NERD = non-erosive reflux disease: The patient often has reflux complaints but does not show any signs of esophagitis in the endoscopic findings.
- ERD = erosive reflux disease (K21.0): The patient has a reflux disease with esophagitis.
40 % of GERD patients have concurrent esophageal lesions. 5 % of these patients develop epithelial dysplasia of the esophagus, which is referred to as Barrett’s esophagus.
Barrett’s esophagus
The esophageal epithelium reacts with epithelial dysplasia to the chronic reflux of gastric acid: The actually stratified uncornified epithelium is replaced by columnar epithelium. Epithelial dysplasia is considered a precancerosis since the development for adenocarcinomas is more likely.

Image: “Micrograph of Barrett’s esophagus” by Nephron. License: CC BY-SA 3.0
Causes of GERD
The most frequent cause is insufficiency of the inferior esophageal sphincter. Further promoting factors are:
- Progressed pregnancy
- Abdominal obesity
- Previous surgical treatment of achalasia
- Stenosis of the gastric exit
- Scleroderma
- Sliding (gliding) hernia
Symptoms of GERD
The most prominent symptom of gastro-esophageal reflux disease is pyrosis. Also, meteorism and flatulence as well as eructating can be observed as rather unspecific symptoms. Due to the increased reflux of the acid at night, hoarseness can be noted in the morning. Reflux-induced vagal irritation leads to dry, irritating cough.
Diagnosis of GERD
- Endoscopy with biopsy for assessment of the inflammatory stages
- 24-hour pH-metry via nasal tube
- Capsule-based pH-metry
Treatment of GERD
Frequent complaints and esophagitis make medication necessary, with proton pump inhibitors like, e.g., omeprazole or pantoprazole being the first-line treatment since the mucosa can regenerate when the acid is suppressed.
H2-receptor antagonists and antacids are only recommended in case of mild symptoms without inflammatory signs. Generally, any treatment of reflux disease should be enhanced by the adhering to the following measures:
- Consumption of acidic and alcoholic beverages like coffee, juice, and wine should be avoided.
- Nicotine abstention
- No late meals
- Avoiding fatty, very sugary food
- Sleeping with elevated head
- Avoiding stress
A laparoscopic Nissen fundoplication, in which a cuff is positioned around the inferior esophageal sphincter, is only indicated if conservative measures have not been successful.
Esophagitis
Symptoms of esophagitis
Symptoms include dysphagia, odynophagia, and retrosternal pain.
Infectious esophagitis
A severe general disease can be accompanied by esophagitis. For example, an infection with Candida albicans can lead to thrush esophagitis, which shows the typical endoscopic picture of numerous white plaques that cannot be wiped away. In immunosuppressed patients, AIDS– and tumor patients, herpes viruses (HSV and CMV) can also trigger esophagitis.
Eosinophilic esophagitis
As part of allergic diseases, this form of esophagitis can be found frequently in children. Endoscopically, eosinophilic infiltration of the esophagus can be seen as whitish papules. Treatment consists of corticoid preparations since in most cases, eosinophilic esophagitis does not respond to PPIs.
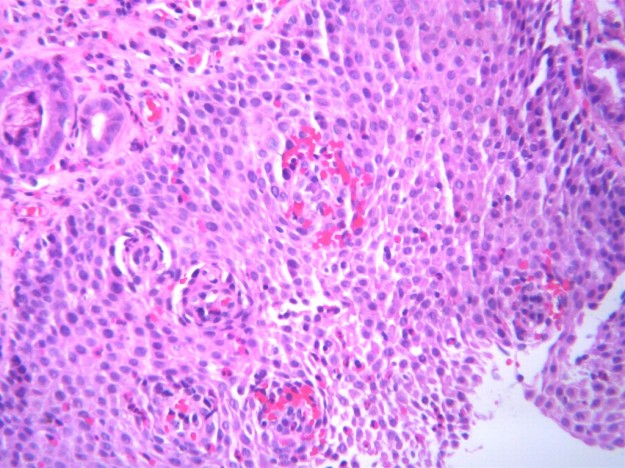
Image: “Eosinophilic oesophagitis, histologic features” by Mattopaedia. License: CC BY-SA 3.0
AIDS and esophageal diseases
In the context of fully developed AIDS, numerous esophageal diseases can develop:
- Thrush esophagitis
- Ulcer formation in cases of infections with the herpes simplex or the cytomegaly virus
- Stenosis of the esophagus with bleedings and perforations through Kaposi’s carcinoma
Other causes of esophagitis
- Chemical causes: chemical burns, reflux of gastric acid = reflux esophagitis, alcohol abuse, medication
- Physical causes: consequences of radiation therapy, gastric tube
- Stenosis: retention esophagitis in cases of achalasia, tumorous processes
Treatment of esophagitis
Depending on the underlying disease, the triggering factors will be treated. This way, reflux esophagitis is treated with proton pump inhibitors, antimycotics are given for thrush esophagitis, and antiviral medications are prescribed in case of HSV- and CMV-associated inflammations.
Tumors of the Esophagus
Benign esophageal tumors
Benign tumors of the esophagus are rather rare and frequently symptom-free. They can growintramurally or intraluminally. They are diagnosed with the esophagus-barium swallow, endoscopy, and endosonography. Smaller intraluminal tumors can usually be eliminated endoscopically with the diathermic sling – larger ones are surgically excised.
Esophageal carcinoma
The malignant neoplasms of the esophagus are squamous epithelial or adenocarcinomas, originating from the epithelium. With 2 % of all cancer diseases, the esophageal carcinoma is relatively rare in Western industrial countries. Men are more frequently affected than women in the sixth and seventh decade of life. Adenocarcinoma of the esophagus develop from a Barrett’s esophagus after a chronic esophagitis.
Triggering factors of squamous epithelial carcinomas include: nitrosamines, aflatoxins, long-lasting consumption of highly concentrated alcohol and very hot food and beverages as well as smoking. Furthermore, chemical burn scars, achalasia, and the Plummer-Vinson syndrome can promote the formation of an esophageal carcinoma.
Symptoms of esophageal carcinoma
Esophageal tumors are often found rather late as they manifest with relatively unspecific symptoms:
- Retrosternal pain, back pain
- Dysphagia
- Regurgitation
- Singultus in case of an infiltration of the vagus nerve
- Hoarseness in case of an infiltration of the recurrent laryngeal nerve
- Irritating cough and other pulmonary symptoms
- Hematemesis
Accompanying symptoms are weight loss, night sweat, and decreased stress resistance.
Pathology of esophageal carcinoma
Predilection sites for carcinoma formation are the three physiologically narrow areas of the esophagus. Both carcinomas spread intraluminal, infiltrate, and metastasize early.

Image: “Endoscopic image of patient with esophageal adenocarcinoma seen at gastro-esophageal junction.” by Samir. License: CC BY-SA 3.0
Staging of esophageal carcinoma
Tumor stages are calssified according to the TNM classification. At the time of diagnosis, these tumors are mostly already in stage III or IV since they remain symptom-free for a long time.
Diagnosis of esophageal carcinoma
- Endoscopy and histology of the biopsy material
- Endosonography for assessment of T- and N-stage
- Sonography of the abdomen
- Chest x-ray
- Bronchoscopy
- CAT
Treatment of esophageal carcinoma
The choice of treatment depends on the stage of the disease:
- Endoscopic abrasion of early adenocarcinomas with high healing rate
- Esophageal resection with stomach elevation and radio-/chemotherapy
- Only radio-/chemotherapy if surgery is no longer feasible
Palliative therapy for the maintenance of food passage includes the implantation of a metal stent for opening the esophageal lumen and laser coagulation.
Overall, prognosis is rather bad since the first noticeable symptom of the disease, dysphagia, is a late symptom already. At the time the diagnosis is made, for 95 % of the tumors, palliative treatment is the only treatment option left.
Emergencies
Rupture of esophageal varice
Portal hypertension with different types of genesis causes the formation of portocaval anastomoses and can thus lead to the development of esophageal varices. These varices can rupture, which very quickly reaches a life-threatening state due to the fulminant bleeding. Therapeutically, the following interventions are available:
- Stabilize circulation (peripheral access, erythrocyte concentrations)
- Possibly a tracheal tube
- Administration of terlipressin, a vasopressin analog
- Application of octreotide, a somatostatin analog
- Antibiotic prophylaxis
- Elastic ligatures, sclerotherapy, or obliteration of the varices
In 10 % of the cases, the bleeding persists and makes further measures necessary. Also, the risk for recurrences is relatively high at 80 %.
Chemical burns of the esophagus with acids and bases
The contact of the mucosa with acids and bases leads to deep necroses, from which inflammations can reactively develop, possibly causing a shock in the patient. Thus, sufficient volume has to be substituted. Also, the esophagus can perforate, which carries the risk of mediastinitis. The differentiation between alkaline and acidic chemical burns occurs with the help of litmus stripes.
Chemical burns are classified according to the degree of severity. A third-degree burn makes a resection of parts of the esophagus necessary because, if all wall layers are completely destroyed, there is always the risk of perforation with all of its sequelae.
Classification of the severity of chemical burns in four stages
- Degree I: Reddening and formation of edema
- Degree II: Mucous ulcers with fibrin plaques
- Degree III: Deep necroses
- Degree IV: Perforation
Boerhaave’s syndrome
Boerhaave’s syndrome refers to the spontaneous rupture of the esophagus after an acute strain through pressure (severe vomiting or choking), which involves the possible complication of a mediastinitis with generalized sepsis. Treatment consists of endoscopic fibrin sealing or a temporary endoprosthetic treatment of the defect, abrosia, and administrationof antibiotics.
Review Questions
Solutions can be found below the references.
1. Which statement concerning esophageal diverticula is not correct?
- Pulsion diverticula are pseudodiverticula.
- The area of Laimer’s triangle and the area above the diaphragm are predilection sites for pulsion diverticula.
- The area of Killian’s triangle is a predilection site for esophageal diverticula.
- Traction diverticula often develop as a consequence of inflammatory processes in the proximity of the esophagus.
- In clinically relevant cases, a resection of the diverticulum is performed.
2. Which statement concerning esophageal carcinoma is not correct?
- Coughing and hoarseness can be symptoms of esophageal carcinomas.
- Barrett’s esophagus, a complication of esophagitis, can lead to the formation of adenocarcinomas in the esophagus.
- Nitrosamines, aflatoxins, concentrated alcohol, and smoking are etiological factors that can lead to squamous epithelial carcinoma in the area of the esophagus.
- The esophageal carcinoma is usually detected early due to its specific symptoms.
- Dysphagia is a late sequela of esophageal carcinoma.
3. Which statement concerning achalasia is not correct?
- It is a neuromuscular disease which is characterized by disorders of the esophageal peristalsis and by the lack of closure of the inferior esophageal sphincter.
- It can be caused by a malignant disease.
- It is treated, amongst other things, with the nervous toxin botulinum toxin.
- If conservative treatment methods fail, it is treated surgically. The most frequent complication is a post-surgical developing reflux disease.
- It manifests mostly as dysphagia and regurgitation of food.



Comentários
Enviar um comentário