Septic Arthritis in Children — Definition and Treatment
Table of Contents

Image : “Going to hospital with Scott” by Marc van der Chijs. License: CC BY-ND 2.0
Definition of Septic Arthritis in Children
Septic arthritis can be defined as the inflammatory condition of the joints that is caused by microbial agents, i.e. bacteria, or less commonly fungi. While septic arthritis is a term that means an infection that is confined to the joints space, the condition usually presents as a complication of osteomyelitis.
Epidemiology of Septic Arthritis in Children
The incidence of septic arthritis has reduced dramatically due to the prompt use of antibiotics in the last few decades. The condition, however, remains more common in children compared to adults.
The condition has become so rare that in a recent study of over four years duration, 34 cases were diagnosed in the United States. The most likely cause of this decline in incidence is the introduction of Haemophilus influenzae type B vaccination. Haemophilus influenzae type B is the most common etiology of septic arthritis in children.
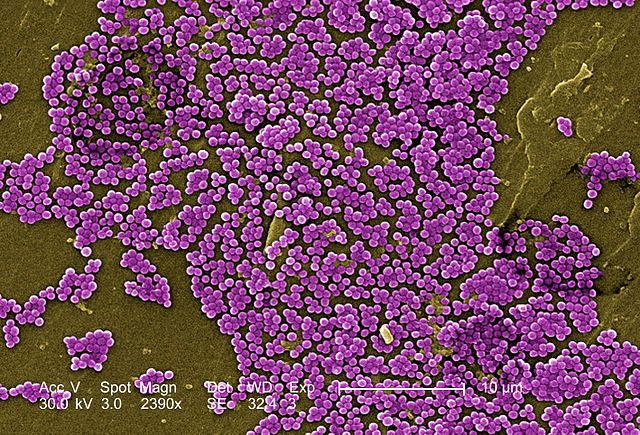
Image: “This colorized 2005 scanning electron micrograph (SEM) depicted numerous clumps of methicillin-resistant Staphylococcus aureus bacteria, commonly referred to by the acronym, MRSA; Magnified 2390x.” by CDC / Jeff Hageman, M.H.S. / Janice Haney Carr – This media comes from the Centers for Disease Control and Prevention’s Public Health Image Library (PHIL), with identification number #10047. License: Public Domain
In the recent years, methicillin-resistant staphylococcus aureus has emerged in the community. Some experts fear that the risk of septic arthritis might increase in the coming years because of the emergence of this antibiotic-resistant bacterium in the community.
There are certain subgroups who are more likely to develop septic arthritis compared to the normal and healthy population. The immunocompromised, children infected with immunodeficiency virus and those with sickle cell anemia are examples of high-risk populations for septic arthritis. Patients with hemophilia are also at risk of developing septic arthritis as a complicated to recurrent hemarthrosis, bleeding inside the joints. The most commonly affected sites of Septic arthritis are large joints of lower limbs. Children belonging to low income families are more likely to develop the disease mostly in age group 0-4 years.
Whether boys are more likely to develop septic arthritis than girls is still debatable. Due to the small number of cases, any statistical conclusions are usually difficult to be made.
Etiology of Septic Arthritis in Children
Bacterial organisms might gain access to the joint space either by hematogenous spread or bydirect invasion of the synovium.
The most likely causative organisms are different according to the child’s age. Children who are younger than two months can develop staphylococcus aureus arthritis, group B streptococci, or other gram-negative bacilli related arthritis.
Before the introduction of Haemophilus influenzae type b vaccination, it was the most common cause of septic arthritis in children aged between two months and five years. The most common cause nowadays in this age group is staphylococcus aureus. Because of this, the recent trend of increased community acquired infections caused by methicillin-resistant staphylococcus aureus is feared to result in a mirrored increase in the incidence of septic arthritis.
Adolescents who develop septic arthritis might have Neisseria gonorrhoeae as the etiology. Children who have sickle cell disease might develop Salmonella osteomyelitis or septic arthritis.
Mycobacterium tuberculosis rarely cause chronic pyogenic arthritis.
Clinical Presentation of Septic Arthritis in Children
Patients with septic arthritis who are old enough to communicate complain of intense joint painthat can be in a single joint or less commonly in multiple joints usually elbow or lower extremity joints especially knee and hip. Pain caused by the disease is so severe that the child cannot tolerate even slight movement of the affected joint. The affected joint is usually swollen and very tender to touch. If joints in the lower extremities are affected, the patient might develop a limp or become unable to bear weight on their legs and avoid walking.
Neonates who develop septic arthritis usually have associated osteomyelitis and multiple joint involvement.
The affected joint is usually very tender and almost complete loss of range of motion around that joint can be evident. This presentation is known as pseudoparalysis. Because of this phenomenon, children usually refuse to walk or bear weight on the affected joints especially if the hip joint is involved. Fever is a very common finding in people with septic arthritis.
Physical examination
Physical examination is very important in the evaluation of the patient with septic arthritis. Decreased or complete absence of range of motion of the affected joint due to severe pain is common. The affected joint is usually swollen, warm to touch and can be red in color. The hip joint if infected is less likely to cause swelling and erythema.
Fever is usually low-grade but is usually present. In some cases, fever might be absent. Children who present with severe pain in a swollen joint are very likely to have septic arthritis and the diagnosis should not be excluded based on the mere absence of fever.
Diagnostic Workup for Septic Arthritis in Children
- In addition to the typical clinical picture, patients with septic arthritis should also have a synovial fluid analysis by synovial culture. Arthrocentesisshould be used to establish the diagnosis in any patient who presents with painful monoarthritis despite the risk of introducing organisms in a sterile joint.
- Septic arthritis is characterized by a white blood cell countof more than 50,000/mL in the synovial fluid. The white blood cell count is usually more than 100,000 per mL with a clear shift to neutrophils. The glucose content in the synovial fluid is usually 30 % of that in the serum,this is another important finding in septic arthritis.
- Erythrocyte sedimentation rate is elevated in patients with septic arthritis. C-reactive protein is also elevated in children with septic arthritis
While synovial fluid culture can provide definite information to establish the diagnosis of septic arthritis, the sensitivity and specificity is considered low. Polymerase chain reaction testing on the other hand can provide reliable information about the presence of a certain causative organism in a reasonable time frame.
5. X-rays of the joint are more helpful in excluding other causes of joint pain such as osteomyelitis rather than establishing the diagnosis of septic arthritis.
6. Ultrasonography of the affected joint is perhaps one of the best diagnostic modalities to establish the diagnosis of septic arthritis. The most common finding on ultrasonography of the joint is the presence of effusions. If an effusion is identified, ultrasound-guided aspiration of the joint’s effusion is indicated.
Treatment of Septic Arthritis in Children
Management of septic arthritis in children should be provided in an inpatient setting. The patient should be admitted to the hospital, intravenous antibiotics should be started and joint immobilization should be used. Joint immobilization should be limited to a maximum of three days, after which, passive range of motion exercises are recommended.
The duration of antibiotic use differs according to the causative organism, which can be predicted based on the patient’s age. Patients who are more likely to have staphylococcal, haemophilus influenzae, or streptococcus pneumoniae as the etiology of their septic arthritis should receive antibiotics for three to four weeks. Adolescents with gonococcal septic arthritis should receive antibiotic therapy for up to ten days.
Image: “Skeletal formula of oxacillin.” by Fvasconcellos – Own work. License: Public Domain
It is clear that the patient is going to receive antibiotics for a long duration. Therefore, the current recommendation is to start intravenous antibiotics for few days until the patient shows good clinical improvement, and then to switch to oral antibiotics.
The antibiotic of choice for neonates with septic arthritis is oxacillin plus gentamicin. Older children who most likely have staphylococcus related septic arthritis should receive oxacillin alone. If the child is suspted to have methicillin-resistant staphylococcus aureus, clindamycin should be used instead of oxacillin.
Cephalosporins are usually used for the treatment of gonococcal septic arthritis in affected adolescents.



{kind=link}
{kind=link}
Comentários
Enviar um comentário