Fetal Malpresentation — Causes and Management
Table of Contents

Image: “Fetus and placenta.” (Image credit: Wei Hsu and Shang-Yi Chiu) – Lessons on Life from SENP2 Sedwick C PLoS Biology Vol. 6, No. 12, e312 doi:10.1371/journal.pbio.0060312. License: CC BY 2.5
Fetal Malposition vs. Fetal Malpresentation
Fetal malposition refers to abnormal fetal vertex positions in relation to the maternal pelvis.
Fetal malpresentation refers to all fetal presentations besides the vertex (occipito-anterior) presentation.
Risk factors for fetal malpresentation
- Multiparity
- Multiple pregnancies
- Prematurity
- Uterine abnormalities like leiomyomas or uterine septa
- Fetal anomalies like polyhydramnios
- Placental anomalies like placenta prevue
- Malpresentation in a previous pregnancy
- Platypelloid and android pelvis.
Breech Presentation
In early pregnancy, the fetus is often in a breech position but, by 36 weeks of pregnancy, it assumes the vertex position, but, when this does not occur and the fetus is positioned with buttocks in the maternal pelvis, it is called a breech presentation. It is the commonest malpresentation in clinical obstetric practice and is usually diagnosed antenatally but may also be diagnosed during labor when the fetal parts are felt through the open cervical os. The incidence of breech presentation is high in cases of premature labor. Variations of breech presentation are:
- Frank breech: in this presentation, the fetal hips are flexed, the knees are extended stretching the legs straight upwards with the head or face lying near the feet.
- Footling breech: here, the baby’s one or both feet lie over the cervix or prolapse through the uterine cervix.
- Complete breech: in this presentation, the fetus lies with both its hips and the knees flexed.
Diagnosis of breech presentation
Antenatally, it can be diagnosed with an ultrasound or it can even be palpated through the maternal abdominal wall by a skilled physician/midwife. Occasionally, the diagnosis of the presentation may be missed or delayed and may only be detected during labor.
Management of breech delivery
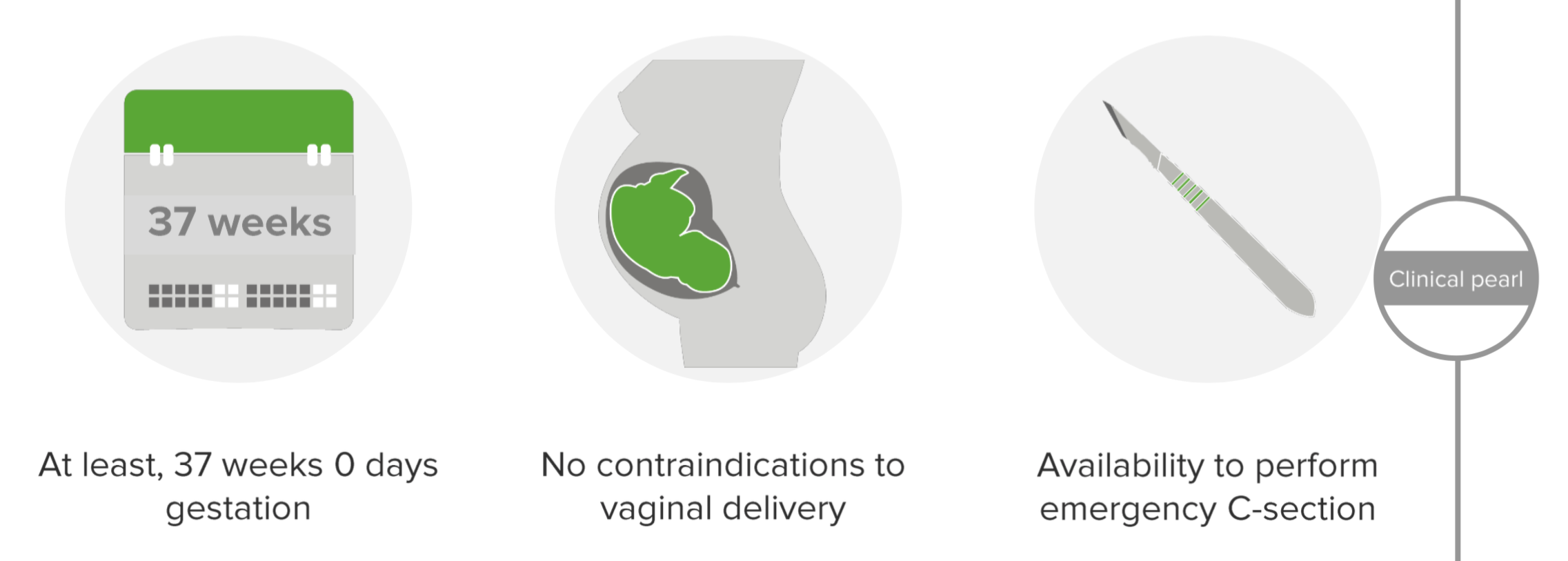
If the presentation is known beforehand, then delivery of the baby should be scheduled in a healthcare facility where surgical intervention, if indicated, can be performed. After 37 weeks of gestation when the woman is in early labor, external cephalic version can be attempted if vaginal delivery is deemed possible, if it is a single gestation, if membranes are intact, if the fetus has no growth retardation or anomalies, and there is no vaginal bleeding or history of a previous cesarean section.
Picture: Criteria for performing external cephalic version
Risks associated with external cephalic version
- Placental abruption
- Rupture of membranes
- Cord prolapse
- Fetal distress
- Fetal hemorrhage
Vaginal delivery can proceed if external cephalic version is successful. If it is unsuccessful, then either a vaginal breech delivery should be attempted, or a cesarean delivery scheduled immediately.
Vaginal breech delivery
This can be attempted in frank or complete breech when the fetus is not too big and there is no maternal cephalopelvic disproportion. Important to remember:
- Watch for cord prolapse
- Meconium is not uncommon in breech deliveries
- Ask patient to push only after confirming with vaginal examination that the cervix is fully dilated
- In the case of fetal distress, or prolonged labor then deliver through cesarean section.
Cesarean section
Cesarean section is indicated in the presence of maternal cephalopelvic disproportion, double footling breech, breech with hyperextended head, a previous history of cesarean delivery and fetal macrosomia.
Complications of breech presentation during labor are cord prolapse with fetal asphyxia or cord compression, fetal head arrest, and fetal trauma.
Face Presentation
Here the fetal face presents with complete head extension. This type of malpresentation is associated with fewer problems during labor, especially if the head flexes during descent in the chin (mentum) anterior position.
However, in the chin/mentum posterior position, the maternal sacrum blocks the fully extended fetal head preventing descent and results in arrest of labor. This can lead to prolonged labor and cesarean section delivery. It is important not to attempt vacuum extraction in a face presentation.
Brow Presentation
In this presentation, the fetal head is partly extended and partly flexed with the mentovertical diameter presenting in relation to the maternal pelvis. It is usually diagnosed when the anterior fontanelle and supraorbital ridges are palpated during a vaginal examination in advanced labor.
Brow presentation often corrects itself during labor and therefore rarely requires a cesarean section to deliver the baby, but if the head does not flex adequately, then a cesarean section has to be performed.
Transverse Lie
In this type of fetal presentation, the fetal head lies transversely across the maternal pelvis with head on one side of the pelvis and buttocks on the other side. These cases are associated with a shoulder presentation, high incidence of cord prolapse and consequent fetal compromiseduring labor so vaginal delivery is not attempted and cesarean section recommended in all such presentations.
Compound Presentation
In this type of fetal presentation, a fetal limb presents along with another fetal part (e.g. vertex) which is closest to the dilated cervical os. Commonly, this involves a fetal arm or hand along with the vertex and rarely the breech and is encountered usually in cases after the premature rupture of membranes or in premature labor or with concomitant pelvic masses.
In these cases, it may occasionally be possible to replace the prolapsed limb. Excessive force should not be applied to the prolapsed limb as it may cause limb injury or brachial plexus injury (Klumpke’s paralysis) or Horner’s syndrome, or may displace the vertex and entrap the fetus converting it into a difficult shoulder presentation. However, in a majority of the cases, spontaneous vaginal delivery only occurs if the fetus is small or dead and cesarean section is the preferred modality of delivery.



{kind=link}
Comentários
Enviar um comentário