Ovarian Torsion (Adnexal Torsion) — Diagnosis and Treatment
Table of Contents
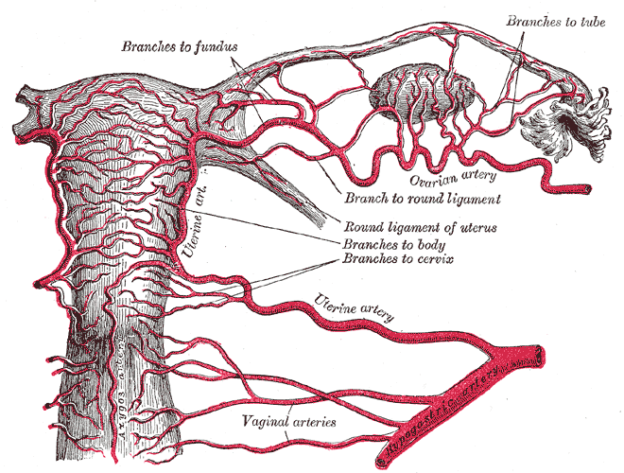
Image : “Gray1170” by Henry Gray. License: Public Domain
Gynecological Anatomy Related to Ovarian Torsion
The infundibulopelvic ligaments are responsible for the suspension of the mobile ovaries. They are responsible for positioning the ovary in a lateral or posterior aspect compared to the uterus. Within these ligaments, the ovarian vessels travel to supply the ovary with blood. The infundibulopelvic ligaments are not fixed; therefore, a tumorous growth can lead to twisting of the ligaments.
The ovary is attached to the uterus by the utero-ovarian ligament. The ligament is composed of muscular and fibrous tissue. This ligament is responsible for providing support to the ovaries preventing twisting. Moreover, blood vessels that arise from the uterine artery also travel along the utero-ovarian ligament to supply the ovaries.
Pathogenesis of Ovarian Torsion
The most common precipitating factor for ovarian torsion is the presence of an ovarian cyst or mass which rotates the ovary around the infundibulopelvic and utero-ovarian ligaments. In most cases, the ovarian mass or cyst is a benign tumorous growth rather than a malignant one.
Torsion is also seen in pre-menarchal girls who do not have any ovarian abnormalities. The most likely cause of ovarian torsion in this age group is the normal physiologic elongation of the infundibulopelvic ligaments. The length of the infundibulopelvic ligaments shortens as the girl enters puberty.
Epidemiology of Ovarian Torsion
Ovarian torsion is the most common cause of gynecological surgical emergencies.
Up to 2.7% of women with adnexal torsion have ovarian torsion; whereas, 15% of women with an ovarian mass who are treated surgically were found to have ovarian torsion.
Most ovarian torsions occur in women in the reproductive age; however, up to 17% of the cases of ovarian torsion were found in pre-menarchal or post-menopausal women.
Risk Factors
The most important risk factor for ovarian torsion is ovarian mass. Up to 80% of the cases of ovarian torsion are associated with a history of an ovarian mass or cyst. The size of the mass is positively correlated with the risk of ovarian torsion. The average diameter of ovarian masses in patients with ovarian torsion was found to be around 9.5 cm.
Ovarian cysts are more likely to occur in women with benign ovarian masses, rather than in those with malignancy. The estimated incidence of ovarian torsion in women with ovarian malignancy was found to be below 2%.

Ovarian stimulation is shown to increase the risk for developing torsion mainly due to the ability to lead into development of a mass/ cyst.
The second risk factor for ovarian torsion is the age of the patient. Pre-menarchal girls have an increased risk of ovarian torsion of normally appearing ovaries, compared to women in the reproductive age who also have normal appearing ovaries.
Up to 22% of ovarian torsions occur in pregnancy. The incidence is highest in pregnant women who are at 10 to 17 weeks of gestation, especially if they have an ovarian mass.
Other risk factors for development of ovarian torsion include:
Congenital abnormalities, such as an elongated fallopian tube.
A history of pelvic surgery may indicate the presence of adhesions that may trigger the formation of ovarian torsions.
Clinical Presentation of Ovarian Torsion
The most common symptom of ovarian torsion is:
- Acute lower abdominal pain.
- Nausea (continuous or comes and go in waves) and vomiting.
- Sudden and severe pain.
Pre-menarchal girls usually develop diffuse pain rather than localized lower abdominal pain. Patients might also develop a low-grade fever.
There may be a history of recurrent episodes of similar events indicating a self-resolving state.
Fever may set in after necrosis of the organ or super infection of the edematous tissue.
Further examination shows an adnexal mass in 50% of the patients and tender abdomen in 30% of the patients. Lack of one or both doesn’t rule out ovarian torsion.
Diagnostic Workup for Ovarian Torsion
Once a thorough history and physical examination is obtained, laboratory testing should be started. Serum human chorionic gonadotropin levels should be determined to exclude ectopic pregnancy as a cause of acute abdominal pain.
Hematocrit, white blood cell count, and electrolytes should be evaluated in all patients presenting with an acute abdomen, including those presenting with acute ovarian torsion.
Also helpful in the diagnostic workup for ovarian torsion:
- Serum markers
- Imaging studies
- Ultrasonography
- Magnetic resonance imaging
- Visualization during surgery
Serum markers can hint to the possibility of an adnexal mass; however, there are no specific serum markers that are suggestive of torsion. Serum human chorionic gonadotropin levels are usually elevated in women with ovarian germ cell tumors. CA-125 levels are elevated in women with malignant ovarian tumors. Patients with ovarian torsion might have an elevated serum level of interleukin-6.
Imaging studies are important in the evaluation of any patient presenting with a suspected pelvic mass. Ultrasonography is the first-line diagnostic imaging modality. A torsed ovary appears rounded and enlarged compared with the contralateral ovary. The enlargement of the ovary is due to edema and vascular engorgement.
Ultrasonography is also useful in the evaluation of ovarian masses as it can define the components, location and density of the mass. Doppler flow is helpful in the evaluation of the blood supply compromise in the case of ovarian torsion.
Magnetic resonance imaging is helpful in the diagnosis of ovarian torsion when ultrasonography is inconclusive. Moreover, magnetic resonance imaging is helpful in differentiating between the different types of ovarian cysts and masses. Computed tomography is not helpful in confirming the diagnosis of ovarian torsion; however, it can exclude other causes of acute abdominal pain, such as acute appendicitis.
Treatment of Ovarian Torsion
Ovarian torsion is a surgical emergency. The laparoscopic approach has become the popular choice in patients with ovarian torsion and no clues of malignancy. If malignant disease is suspected, a laparotomy should be performed.
During the surgery, it is essential to assess the viability of the ovary. Early de-twisting of the ovary can preserve the function of the ovary. Viability is determined by gross visual inspection during surgery. Nowadays, ovarian preservation surgery is always recommended, even if the ovary appears black or blue. Salpingo-oophorectomy should be avoided whenever possible.
Ovarian cystectomy is performed to excise the benign ovarian mass, which was responsible for the torsion. If malignancy is suspected, a salpingo-oophorectomy might be performed.
Necrosis typically occurs after the ovarian vessels have been occluded for 36 hours or more. Accordingly, early intervention to save the ovaries is recommended. Pregnant women with ovarian torsion should undergo laparoscopic detorsion like non-pregnant women.
Suppression of ovarian cysts by the administration of oral contraceptives and oophoropexy are the most common options for the prevention of recurrence after detorsion. Patients with ovarian torsion typically are in severe pain; therefore, good analgesia is recommended while at the emergency department before transferring the patient to the operating theater.



{kind=link}
{kind=link}
Comentários
Enviar um comentário