Spinal Cord Pathologies: Multiple Sclerosis (MS), Amyotrophic Lateral Sclerosis (ALS), Poliomyelitis and More
Table of Contents
Definition and Basic Sciences
The spinal cord is a continuation of the central nervous system and starts at C1, which is just below the medulla of the brainstem and extends down to the level of the space between the first and second lumbar vertebrae where it becomes the conus medullaris.
Blood supply is via:
- Vertebral arteries that forms one anterior and two posterior spinal arteries.
- Anterior and posterior radicular arteries that are branches of the intercostal and lumbar vessels.
Etiology of Spinal Cord Pathologies

Image: “Transverse myelitis, This 53 year old woman rapidly developed neurological symptoms, which resolved over the course of weeks. Followup MRI three months later demonstrated significant reduction is the size of the lesion. It is felt to be consistent with transverse myelitis.” by Frank Gaillard – http://radiopaedia.org/cases/transversemyelitis and http://radiopaedia.org/uploads/radio/0001/3690/TM_01.jpg. License: CC BY-SA 3.0
Causes of spinal cord pathologies include:
- Trauma
- Extraspinal masses (including tumor, abscess and hemorrhage)
- Intraspinal mass (including hematoma and tumor)
- Inflammation (e.g., transverse myelitis)
- Nutritional deficiency (B12 deficiency causes dorsal column dysfunction)
- Infection (including Tabes dorsalis from syphilis)
- Vascular (stroke, AVM)
Pathophysiology of Spinal Cord Pathologies
Poliomyelitis and spinal muscular atrophy
Rare set of genetic conditions that cause muscle wasting. Damage seen to the destruction of the anterior (ventral) horns of the spinal cord.
Multiple sclerosis
The precise pathogenesis of the condition is unknown. However, it is an inflammatory autoimmune condition that causes demyelination of seemingly random areas of the spinal cord and brain. It is known to be T cell mediated.
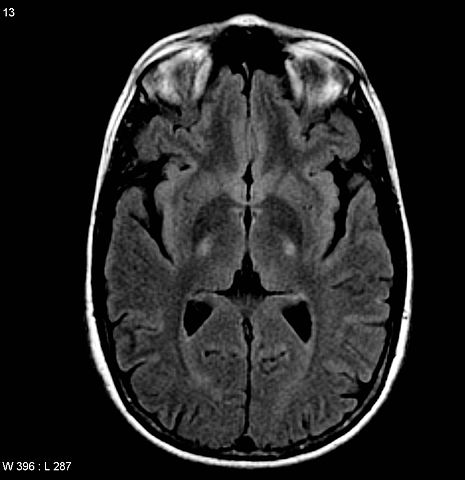
Image: “Amyotrophic lateral sclerosis. MRI (axial FLAIR) demonstrates increased T2 signal within the posterior part of the internal capsule, consistent with the clinical diagnosis of ALS” by Frank Gaillard. License: CC BY-SA 3.0
Amyotrophic lateral sclerosis
ALS affects both upper and lower motor neurons in the CNS (spinal cord, brain and cranial nerve motor nuclei typically). It has an unknown cause. However, it has a hallmark pathology of ubiquitinated TDP-43 and FUS proteins. As such it has an overlap with frontotemporal dementia (FTD) and 5 % of ALS patients will go on to develop FTD. 5 % of cases are familial and due to a mutation in SOD-1 (amongst other genes).
Anterior spinal artery syndrome
This can occur for a number of reasons including trauma, surgery, vasculitis, emboli or severe hypertension. Of specific note is occlusion of the artery of Adamkiewicz, which supplies the T8 level and has relatively poor supply, making it a likely candidate for watershed infarct.
Tabes dorsalis
In the third, tertiary, stage of syphilis, T Pallidum can infect spinal cord neurons and cause degeneration of the axons. Typically, this occurs in the dorsal columns of the spinal cord.
Vitamin B12 deficiency
A spinal cord lesion can be caused by pernicious anaemia as a result of B12 deficiency.
Acute spinal cord compression
This usually causes compression of nerve, resulting in spastic paraparesis. It can occur for a number of reasons including disc prolapse, trauma, tumors of the spinal cord, tuberculosis, spinal abscess and epidural hematoma.
Examples of Spinal Cord Pathologies
Poliomyelitis and spinal muscular atrophy
Patients will show with LMN lesions due to the damage to the ventral horns of the spinal cord. Patients as such have a flaccid paralysis.
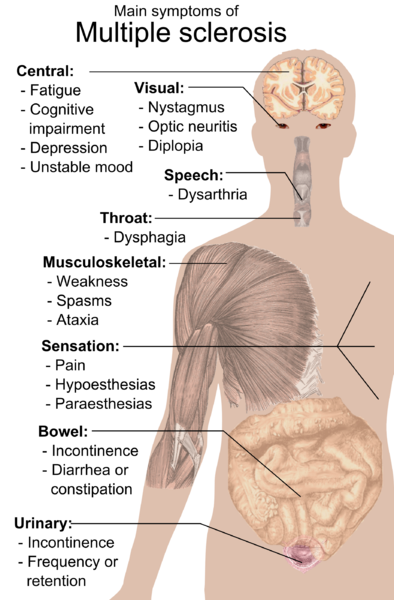
Image: “Main symptoms of Multiple sclerosis.” by Mikael Häggström. License: Public Domain
Multiple sclerosis
Multiple sclerosis can cause spinal cord lesions. Asymmetric lesions mostly of the white matter cause a variable pattern of presentation. No single set of symptoms are diagnostic in multiple sclerosis. However, its relapsing and remitting course is often the key to diagnosis. Patients can experience vertigo, unsteadiness, pain, spasticity or sensory problems.
Work-up: the distinctive feature on MRI imaging is that the lesions do not exceed more than two vertebral bodies.
Amyotrophic lateral sclerosis (ALS)
Can also cause spinal cord lesions. It can present in a number of ways. ALS classically presents with both UMN and LMN lesions in a single limb. Over time it will spread throughout the trunk. A patient may present with tingling and muscle wasting in a hand, before fasciculations develop.
ALS can also present with progressive muscular atrophy where patients get a pure LMN lesion, presenting with muscle weakness wasting and fasciculations usually in a single limb before it spreads.
Spinal cord transection
Spinal cord transection is associated with upper motor neuron signs below the level of the lesion. On examination this will result in spastic paralysis and hyporeflexia. Patients will complain of sensory loss. On examination they will have sensory loss below the level of the spinal cord transection. However, at the level of the lesion the patients may show lower motor neuron signs (as damage to the LMN can take place at the level of the transection).
Central cord syndrome
Patients will have loss of pain and temperature in a “cape like distribution”. Lower motor neuron signs in the arms and upper motor neuron signs in the lower extremities. Central cord syndrome typically spares the dorsal columns. It can arise from syringomyelia, whereby the spinal canal expands due to increased CSF, either from trauma causing blockade or via a tumor in the ventricles or elsewhere.
Patient typically progress over many decades. Surgical decompression of the foramen magnum is a possibility for resolution, as is surgery to remove any tumors
Anterior spinal artery syndrome
Pathophysiology: It is also known as Becks syndrome and may occur for many reasons including trauma, surgery, vasculitis, emboli or severe hypertension. Of specific note is occlusion of the artery of Adamkiewicz, which supplies the T8 level and has relatively poor supply, making it a likely candidate for watershed infarct.
The anterior two thirds of the spinal cord are deprived of their blood supply leading to ischemia and necrosis. Hence the spinothalamic tracts are affected leading to examination findings of spastic paralysis and loss of pain and temperature with intact joint position sense and vibration. This will typically spare the dorsal columns whilst damaging the spinothalamic and corticospinal tracts.
The disease has a 20—50 % chance of survival depending on the severity.

Image: “Demyelinization of the posterior columns of the spinal cord known as “Tabes Dorsalis”, or Tabetic Neurosyphilis. This image shows severe demyelinization of the posterior columns of the spinal cord due to long-standing syphilis disease. This can result in a staggering, wide-based gait, postural instability, pain and paresthesias; Myelin stain; magnification 450X.” by Photo Credit: Content Providers: CDC/Susan Lindsley – This media comes from the Centers for Disease Control and Prevention’s Public Health Image Library (PHIL), with identification number #2345. Note: Not all PHIL images are public domain; be sure to check copyright status and credit authors and content providers. License: Public Domain
Tabes dorsalis
Patients will often have impaired sensation of fine touch. As they have lost the dorsal columns they will also lose proprioceptive abilities and the vibration sense. They may have an inability to feel their legs that has progressively worsened. You may notice on examination that they have poor coordination.
There are a number of associated symptoms that it is key to look out for. Patients will have charcot joints (presumably from inability to feel), shooting pains and crucially the typical Argyll Robertson pupil. These are small pupils that constrict poorly to light.
On examination, a Romberg’s test for balance should be carried out. Patients with Tabes dorsalis will be positive for Romberg’s.
Vitamin B12 deficiency
A spinal cord lesion can be caused by pernicious anemia because of B12 deficiency. This is because the body does not make or store vitamin B12 or the stores get depleted quickly and thus one must depend on dietary supplementation.
Patients will initially feel numbness and tingling of the extremities (i.e. fingers and toes) before sensory loss at the extremities. If left, patients will deteriorate with generalized weakness and dementia eventually developing.
On examination you may find the patients have an absent ankle jerk reflex.
If you suspect the patient may have a B12 deficiency check their activated B12 levels, as well as methylmalonic and homocysteine levels. You can prescribe parenteral B12, which will usually reverse the peripheral nerve damage (remember, peripheral nerves have a different and more effective pattern of regeneration) but damage to the spinal cord and cortex is usually permanent.
Acute spinal cord compression
Patient usually have a chronic or subacute presentation (unless there is significant trauma). Look for spastic paraparesis. Sensory level numbness may be seen. This is defined as loss of sensation from the feet up to 2-3 levels before the level of anatomical compression. Patients will have constipation and urinary retention (due to compression above L2, 3, 4). Swift diagnosis is essential and an MRI should be ordered immediately.
Complications of Spinal Cord Pathologies
Severe complications can result from explorative surgery including hemorrhage and nerve damage. Spinal cord compression can result in long term functional loss if not treated promptly (due to neuronal death).
All forms of spinal cord pathologies can result in long term pathology if neuronal cell death occurs.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comentários
Enviar um comentário