Post Traumatic Stress Disorder (PTSD) — Symptoms and Causes
Table of Contents
- Overview of Post-traumatic Stress Disorder
- Epidemiology of Post-traumatic Stress Disorder
- Etiology and Pathology of Post-traumatic Stress Disorder
- Clinical Presentation of Post-traumatic Stress Disorder
- Diagnostic Workup for Post-traumatic Stress Disorder
- Treatment of Post-traumatic Stress Disorder
- References
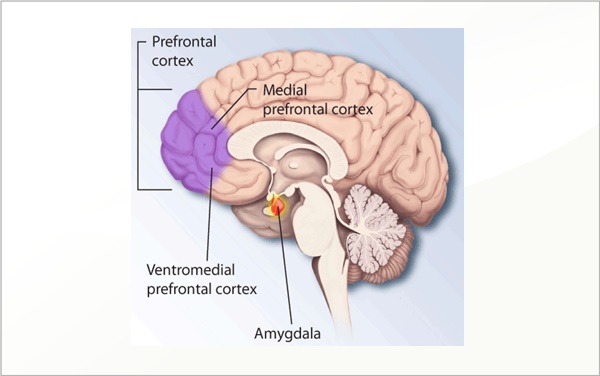
Image: “Ptsd-brain” by National Institutes of Health. License: Public Domain
Overview of Post-traumatic Stress Disorder
Post-traumatic stress disorder is defined as the anxiety disorder that usually develops after someone experiences a severe trauma that is known to constitute a threat to one’s physical well-being or one’s own life. Post-traumatic stress disorder can also happen as a consequence of experiencing a traumatic event that affected another person who is important to the subject even the event is over and they have escaped from danger. It remains under-recognized and untreated in many cases.
Epidemiology of Post-traumatic Stress Disorder
PTSD in both sexes
The estimated prevalence of post-traumatic stress disorder in the U.S. is around 8 – 10%. Women are more likely to develop post-traumatic stress disorder compared to men. Additionally, the nature of the traumatic event is also different between men and women. Sexual assault is the most common trigger for post-traumatic stress disorder in women, whereas trauma from combat is the most common cause of post-traumatic stress disorder in men.
A recent study suggested that the risk of post-traumatic stress disorder is more related to the duration and severity of the experienced trauma rather than the individual’s sex. Post-traumatic stress disorder can be diagnosed in all age groups. The estimated prevalence of post-traumatic stress disorder in adolescent males is around 3.7%, whereas the prevalence of the disorder in adolescent females is around 6.3%.
Types of Risk Factors that lead to PTSD
- Sexual violence relationship: Rape, childhood sexual abuse, intimate partner violence
- Interpersonal-network traumatic experiences: Unexpected death of loved one, life-threatening illness of a child, other traumatic events of a loved one
- Interpersonal violence: Childhood physical abuse or witnessing interpersonal violence, physical assault, or being threatened by violence
- Exposure to organized violence: Refugee, kidnapped, civilian in a war zone
- Participation in organized violence: Combat exposure, witnessing death/serious injury or discovered dead bodies, accidentally or purposefully caused death or serious injury
- Other: Life-threatening motor vehicle collision, natural disaster, toxic chemical exposure
The prognosis of PTSD
The prognosis of post-traumatic stress disorder in treated patients is good with complete or almost complete recovery in most cases. Rapid involvement with treatment, social support, avoidance of re-experience of any trauma and the absence of other psychiatric disorders or substance abuse are good prognostic factors in post-traumatic stress disorder. If the disorder is not treated well, there is a predisposition of personality disorders, drug or substance abuse, affective disorders and other medical problems.
Etiology and Pathology of Post-traumatic Stress Disorder
Symptoms of post-traumatic stress disorder usually happen within three months after the traumatic event.
Many of the symptoms of post-traumatic stress disorder can be explained by the activation of these brain regions. The orbitoprefrontal cortex plays a critical role in inhibiting the over-activation of these brain regions in normal subjects. Patients with post-traumatic stress disorder show decreased inhibition by the orbitoprefrontal cortex and alteration in functioning of the hypothalamic pituitary axis.
Clinical Presentation of Post-traumatic Stress Disorder
The diagnosis of post-traumatic stress disorder is based on 8 criteria from the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5):
Patients should directly experience the traumatic event or should witness the traumatic event when it affected another person. Sometimes, patients might know about the traumatic event that a close family member has encountered but not witness it. In most cases of post-traumatic stress disorder, the exposure to the traumatic event is repeated and extreme. In some cases, there is indirect exposure to aversive details of the traumatic events mostly in course of professional responsibilities.
Patients should have persistent thoughts, images, dreams, nightmares hallucinations, dissociative flashback episodes, or intense distress after experiencing the traumatic event.
Patients also show avoidance behavior where they avoid talking or feelings related to the traumatic event. Additionally, patients usually avoid places and people that might trigger the recollection of the traumatic event.
Patients should also have two or more of the following symptoms to be diagnosed with post-traumatic stress disorder. The inability to remember an important aspect of the triggering event, persistent negative beliefs about oneself, distorted thoughts about the cause of the event, a persistent negative emotional state, a markedly diminished interest in participation in daily activities, feeling of isolation and the inability to experience positive emotions are included in this criterion.
Patients should also have two or more symptoms that are suggestive of altered arousal. Examples of such symptoms include anger outbursts, self-destructive behavior, hypervigilance, concentration problems, excess startle reactions and sleep disturbances.
The duration of these symptoms should be more than one month; the symptoms should significantly impair the quality of life for the patient, and proper exclusion of medical conditions or drug abuse as causes of the symptoms are the three remaining criteria for the diagnosis of post-traumatic stress disorder.
The risk of myocardial infarction has been previously shown to be higher in patients with post-traumatic stress disorder, compared to subjects without a previous history of post-traumatic stress disorder.
The mental status examination in patients with post-traumatic stress disorder might reveal several abnormalities. Mood and concentration are usually impaired. Additionally, memory impairment has been observed in patients with post-traumatic stress disorder. Mental Symptoms related to medication, substance use or other illness are excluded. The risk of concurrent major depressive disorder in women with post-traumatic stress disorder is high.
Diagnostic Workup for Post-traumatic Stress Disorder
Laboratory investigations
Laboratory investigations are not useful in the management of post-traumatic stress disorder but might be indicated for assessment of substance abuse and research purposes. Cortisol levels have been found to be decreased in patients with post-traumatic stress disorder. Elevated levels of norepinephrine and epinephrine are usually seen in patients with this disorder.
Endogenous opiates
Endogenous opiates were found to be elevated in patients with post-traumatic stress disorder and are thought to be related to the blunted emotions seen in patients with post-traumatic stress disorder.
Magnetic resonance imaging studies
Magnetic resonance imaging studies of the brain are also performed for research purposes and to exclude medical conditions that might cause similar symptoms. Hippocampal atrophy is commonly seen in patients with post-traumatic stress disorder. A decrease in size of corpus collosum and prefrontal cortex and increase in reactivity in amygdala and decrease in the action of the prefrontal cortex are observed in imaging studies. Some studies even suggest that the size of the hippocampus might be correlated with the risk of post-traumatic stress disorder later in life.
Treatment of Post-traumatic Stress Disorder
Eye movement desensitization and reprocessing (EDMR)
Eye movement desensitization and reprocessing (EDMR) is thought to activate the different brain regions that are related to information processing and the inhibition of the activated brain regions known to cause the symptoms of post-traumatic stress disorder. Therefore, trauma-oriented cognitive behavioral therapy, when combined with EDMR, has been shown to be successful in managing the symptoms of the condition. This therapy is helpful in shortening the course of recovery.
Pharmacotherapy
Pharmacotherapy might be also indicated, especially in the early stages, to make it possible for the patient to go to work and still be integrated. Use of Benzodiazepine and atypical antipsychotics are not recommended in PTSD.
Beta-blockers
The medical treatment of choice for post-traumatic stress disorder that is not associated with depression is beta-blockers. Alpha-antagonists have also shown some efficacy.
Benzodiazepines should be avoided, if possible, due to the increased risk of drug dependence as it may lengthen the course of PTSD. Patients with comorbid depression usually respond well to antidepressants combined with beta-blockers. Prazosin has been shown to decrease the rate of nightmares and insomnia and lower the severity of the symptoms during the day.
Difference between Acute Stress Disorder and PTSD
Patients who experience a major traumatic event but have anxiety symptoms for only a short duration. To quantify for this diagnosis, the symptoms must occur within 1 month of the trauma and last for a maximum of 1 month. Symptoms are similar to those of PTSD.



{kind=link}
Hey! Thanks for the post. Depression really ruin your life completely. I know this because I gonna through this horrible state of mind. To overcome the depression I searched for the best Counselling in South West London. Finally, I get rid of it. Hey! you have shared really a great post.
ResponderEliminarHello Dear,
ResponderEliminarI Like Your Blog Very Much. I see Daily Your Blog, is A Very Useful For me.
You can also Find PTSD Counselling We offer private counseling for individaul, couples and family. Our experienced psycotherapist provide counseling for anxiety, marriage and depression etc.
Visit Now:- https://edmontoncounsellingservices.ca/