Croup (Laryngotracheobronchitis) — Causes and Treatment
Table of Contents
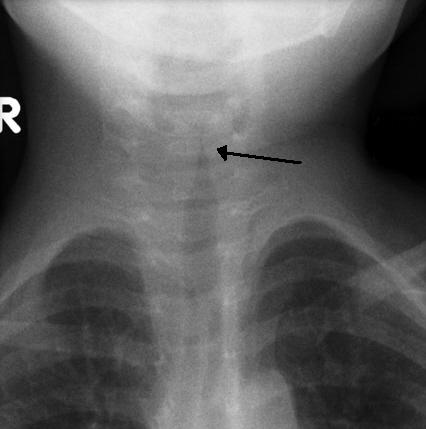
Image: “AP x-ray of the neck in a child with croup demonstrating the steeple sign; narrowing of the the trachea.” by Frank Gaillard – Own work. License: CC BY-SA 3.0
Definition
Croup is a common pediatric disease of upper respiratory tract caused by viral infection rarely by a bacterial infection. It is represented by inflammation of the larynx and trachea that can extend to bronchi interfering with normal breathing, leading to a seal-like barking cough and an inspiratory noise termed as stridor. It is also known as laryngotracheitis or Laryngotracheobronchitis.
Pathophysiology of Croup
The viral infection triggers the infiltration of white blood cells especially histocytes, neutrophils, plasma cells and lymphocytes which ultimately lead to swelling inside trachea, larynx and then large bronchi. The swelling obstructs the airway partially, leading to narrowing of the airway and worsens the case by heavy involvement in breathing during exercises and other vigorous physical activities resulting in a turbulent noisy inspirational airflow termed as stridor.
Epidemiology of Croup
The children in age 6 months to 36 months are primarily affected by croup. The peak incidence of croup occurs in between 6 months to 6 years up to 15 years. 15 % emergency hospitalization of children is caused by croup itself.
The disease is more prevalent in autumn season and affects 50 % of males more than females. It is prevalent in North America where 5-6 cases per 100 toddlers are seen in the second year of their life. It is more common in boys as compared to girls.
Transmission
Croup is contagious within the first few days usually in the first or second day. A virus can be transmitted in the form of droplets released by sneezing and coughing.
Risk Factors of Croup
Season change: change of weather from autumn to winter or winter to spring may trigger the onset of Croup.
Prematurity: the infants above 6 months and children up to the age 6 years are more at the risk.
Young age: below 15 years, children can catch croup.
Asthma: asthma can be another risk factor for the disease.
Viral infection: the causative organism in the disease are parainfluenza, respiratory syncytial virus, metapneumovirus, adenovirus, influenza A and B and mycoplasma
Signs and Symptoms of Croup
- Characteristic barking cough
- Stridor
- Low-grade Fever
- Hoarseness
- Acute enlargement of the tonsils
- Diphtheria
- Difficulting in eating (dysphagia)
- Coryza
- Hoovers’s sign (indrawing of chest wall)
- Agitation
- Trauma
- Tumour in severe cases
Causes and Diagnosis of Croup
Croup is most commonly caused by a virus in 75% of cases and less commonly by bacteria. In most of the cases, the causative agent is parainfluenza virus type 1 and 2, (a member of paramyxovirus family). It can also be caused by measles virus, respiratory syncytial virus (RSV) and adenovirus.
Croup caused by bacteria is divided into:
- Bacterial tracheitis
- Laryngotracheobronchitis
- Laryngeal diphtheria
- Laryngotracheobronchopneumonitis
Corynebacterium diphtheriae causes laryngeal diphtheria while laryngotracheobronchitis, bacterial tracheitis, and laryngotracheobronchopneumonitis are due to secondary bacterial growth.
The most common bacteria associated with croup is:
- Staphylococcus aureus
- Haemophilus influenza
- Streptococcus pneumonia
- Moraxellacatarrhalis
Diagnosis
No specific laboratory tests or imaging procedures is required for croup. Diagnosis can be made by the clinical appearance of a barking cough and stridor. The severity of Croup can be detected by following laboratory tests:
Lateral neck radiograph to rule out any other cause like a peritonsillar abscess. In cases of croup, X-ray usually shows “steeple sign” which reveals narrowing of upper airways. Bronchoscopy may be indicated in patients having recurrent episodes of croup. Generally, laboratory investigations are avoided to postpone unnecessary distress to the child.
Severity
Severity of the disease can be assessed by Westley score.
A total score of equal to or less than 2 indicates mild croup and there are barking cough and hoarseness, no stridor at rest. A total score of 3-5 indicates moderate croup. A total score of 6-11 indicates severe croup, obvious stridor, and obvious chest wall indrawing.
A total score of more than or equal to 12 indicates approaching respiratory failure with prominent symptoms other than barking cough and stridor.
Treatment of Croup
After a complete evaluation of the case by physical and clinical examination, treatment has proceeded. It can be understood by following:
- The child is made to inhale oxygen by “blow-by” method. Usually, the use of mask or nasal formula is avoided as they can upset the child.
- Endocardial intubation may be required in o.2 % cases to reduce narrowing of the airway.
- Corticosteroids, such as dexamethasone and budesonide is given orally or by injection to improve the condition which usually shows its response in 6 to 8 hours.
- Racemic Epinephrine is given by nebulization to control the severity of the case.
- Hot steam or humidified air use does not seem to provide effective relief in croup.
- Cough medicines having dextromethorphan or guaifenesin are avoided.
- Heliox present minimal support to the condition.
- Antiviral neuraminidase inhibitors are given to the patients of severe croup.
Antibiotics are only prescribed in case of primary or secondary bacterial infection. Vancomycin and cefotaxime are prescribed.
Prognosis
Croup is a self-limiting disease usually resolving within a day or two in 80 % of the cases. Most of the cases improve In 3-7 days. Hospitalization of a child is needed only in 5% cases. Croup is a life-threatening illness but it rarely progresses to death, if it does, usually by cardiac arrest.
Complications
- Pneumonia
- Pulmonary edema
- Bacterial tracheitis
- Cyanosis



{kind=link}
Comentários
Enviar um comentário