Thoracic Trauma: Diagnosis and Management
Table of Contents
- Definition of Thoracic Trauma
- Classification of Thoracic Trauma
- The American Association for the Surgery of Trauma (AAST) Injury Scoring Scale for Chest and Heart Injuries
- Pathophysiology of Thoracic Trauma
- Clinical Features of Thoracic Trauma
- Investigations for Thoracic Trauma
- Management of Thoracic Trauma
- Complications of Thoracic Trauma
- References
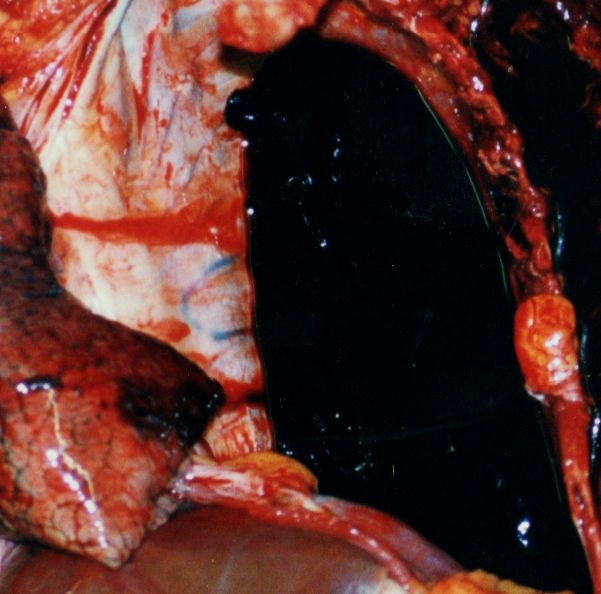
Image: “A diagram of the forces on the brain in concussion.” by Amadalvarez – Own work. License: CC BY-SA 4.0
Definition of Thoracic Trauma
A thoracic traumatic injury can be defined as any form of injury to the chest including the ribs, heart, lungs, and major blood vessels. An injury can be generally classified as blunt or penetrating.
The specific types of chest injuries include injuries to the chest wall, pulmonary injury, airways’ injury, cardiac injury, blood vessel injury, and esophageal injury.
Classification of Thoracic Trauma
By the mechanism of injury
Blunt
Blunt traumatic thoracic injuries are caused by a blunt force trauma to the chest. Blunt trauma can cause contusions, abrasions, lacerations and/or bone fractures.
Penetrating
Penetrating injuries to the thorax happen when an object pierces the skin and enters the chest creating an open wound. The mortality rate of chest penetrating injuries is reported to be under 10%. Penetrating injuries might involve the heart or the major blood vessels within the mediastinum. Lung laceration, pulmonary contusion, hemothorax, pneumothorax, and hemopneumothorax are all more common with penetrating thoracic injuries.
The specific types of chest injuries include:
Injuries to the chest wall
- Rib fractures
- Flail chest
- Sternal fractures
- Chest wall contusions and hematomas
Injuries to the lung
- Pulmonary contusion
- Pulmonary laceration
- Pneumothorax
- Hemothorax
- Hemopneumothorax
Injury to the airways
- Tracheobronchial tear
Cardiac injuries
- Pericardial tamponade
- Myocardial contusion
- Traumatic cardiac arrest
- Hemopericardium
Blood vessel injuries
- Traumatic aortic rupture
- Thoracic aorta injury
- Aortic dissection
Injuries to the esophagus or the diaphragm
By time of required treatment and severity of injury
Major or LETHAL SIX, should be recognized in the primary assessment:
- Airway obstruction
- Tension pneumothorax
- Cardiac tamponade
- Open pneumothorax
- Massive hemothorax
- Flail chest
Minor or HIDDEN SIX, can be unrecognized in primary, but is absolutely necessary not to miss the following:
- Thoracic aortic disruption
- Tracheobronchial disruption
- Myocardial contusion
- Traumatic diaphragmatic tear
- Esophageal disruption
- Pulmonary contusion
The American Association for the Surgery of Trauma (AAST) Injury Scoring Scale for Chest and Heart Injuries
AAST Injury Scoring Scale for Chest Wall Injury
Grade I
- Any size of a chest wall contusion
- Skin and subcutaneous lacerations
- Close fracture of less than 3 ribs or non-displaced closed fracture of the clavicle
Grade II
- Any chest wall laceration that involves the skin, subcutaneous and muscle
- Fracture of three or more adjacent ribs that is closed
- An open or a displaced fracture of the clavicle
- A non-displaced closed fracture of the sternum
- A closed or open fracture of the scapular body
Grade III
- Full thickness laceration with penetration of the pleura
- An open or displaced fracture of the sternum
- A flail sternum
- Unilateral flail chest of less than 3 ribs
Grade IV
- An avulsion laceration of the chest wall tissues with underlying rib fractures
- Unilateral flail chest of three ribs or more
Grade V
- Bilateral flail chest of three ribs or more on both sides
AAST Injury Scoring Scale for Lung Injury
Grade I
- A unilateral lung contusion that involves less than one lobe
Grade II
- A unilateral lung contusion that involves a single lobe
- A lung laceration that is associated with simple pneumothorax
Grade III
- A unilateral lung contusion that involves more than one lobe
- A lung laceration that is associated with persistent air leak for more than 72 hours
- A non-expanding lung hematoma
Grade IV
- Major segmental or lobar air leak
- An expanding lung hematoma
- A vascular injury that involves the primary branches of the intrapulmonary vessels
Grade V
- Disruption of the blood vessels at the lung hilum
Grade VI
- A total transection of the pulmonary hilum
AST Injury Scoring Scale for Heart Injury
Grade I
- Blunt cardiac injury – minor EKG abnormality (nonspecific ST of T wave changes, premature atrial or ventricular contractions, or persistent sinus tachycardia)
- Blunt and/or penetrating pericardial trauma without cardiac injury, including tamponade and/or cardiac herniation
“Malignant cardiac tamponade from non-small cell lung cancer” Image created by Lecturio
Grade II
- Blunt cardiac injury without cardiac failure with heart block or ischemic changes
- Penetrating tangential cardiac wound, not extending through endocardium, no tamponade present
Grade III
- Blunt cardiac injury with sustained/multifocal ventricular contractions
- Blunt or penetrating cardiac injury, combined with rupture of septum, pulmonary or tricuspid incompetence, dysfunction of papillary muscle and/or distal coronary artery occlusion not joined with cardiac failure
- Blunt pericardial laceration combined with cardiac herniation
- Blunt cardiac injury and cardiac failure
- Penetrating tangential myocardial wound, not through endocardium combined with tamponade of the heart
Grade IV
- Blunt or penetrating cardiac injury including rupture of the septum, pulmonary or tricuspid incompetence, dysfunction of papillary muscle, distal coronary artery occlusion leading to cardiac failure
- Blunt or penetrating cardiac injury and aortic or mitral incompetence
- Blunt or penetrating cardiac injury of the right ventricle, right /left atrium
Grade V
- Blunt or penetrating cardiac injury and proximal coronary artery occlusion
- Blunt or penetrating left ventricular perforation
- Stellate injuries, with no more that 50% tissue loss of the right ventricle, right or left atrium
Grade VI
- Blunt avulsion of the heart
- Penetrating wound with more than 50 % tissue loss of chambers
Pathophysiology of Thoracic Trauma
Fractured bones
Ribs, clavicle, and sternum, thoracic vertebrae leading to pain, inadequate ventilation and subsequent complications:
- Clavicle – necessary to exclude trauma of the lung apices and subclavian vessels (chest X-Ray/CT)
- Sternum – potential myocardial contusion and internal thoracic vessels trauma (cardiac echo/CT)
- 1st rib – necessary to exclude trauma of the lung apices, subclavian vessels (chest X-Ray/CT)
- 2nd rib – may be joined with ascending aorta and superior vena cava trauma (CT)
- 10th rib – necessary to exclude diaphragmatic, liver, splenic injury (US/CT)
- 11th rib – necessary to exclude diaphragmatic, liver, splenic injury (US/CT)
- 12th rib – necessary to exclude renal injury (US/CT)
Flail chest
It is a segment of the thoracic cage separated from the rest of the chest wall, usually represented by a free segment (at least two fractures per rib in at least two ribs) that is not contributing to lung expansion and thus is leading to inadequate ventilation. If large enough, it requires mechanical ventilation.
The expansion of the chest wall during inspirations occurs, but the flail chest segment moves inwards because of the sucking effect of negative intrathoracic pressure leading to limited lung expansion and thus ineffective ventilation and hypoxia.
As force is needed to fracture ribs at multiple sites, these injuries are often associated with an extensive lung contusion, complicated by hemothorax and/or pneumothorax. It is the underlying injury that causes respiratory dysfunction, rather than the flail segment itself. If inadequate analgesia is performed, pain makes breathing shallow and worsens the ventilation further leading finally to airway collapse and pneumonia.
Hemothorax
This is the collection of blood in pleural space. If it is a result of rib fracture, lung and minor venous injuries, then it is a self-limiting disease. In fewer cases, an arterial injury is the underlying cause, and requires surgical repair.
Aortic injury
The most serious aortic injury is aortic transection with imminent death. Other options are tear with dissection or pseudoaneurysm formation with potential recovery if cases of adequate management. These scenarios happen due to deceleration injury, when aortic arch and aorta move suddenly within the chest cavity and tear occurs most frequently distal to left subclavian artery origin.
Cardiac trauma
Various injuries of heart that are roughly divided into:
- Penetrating trauma presenting as cardiac tamponade: blood or other fluid rapidly collects in pericardial space, restricts cardiac motion, lowers output and leads to cardiac arrest and death if not managed promptly.
- Blunt cardiac trauma: Difficult to diagnose due to the absence of laboratory testing and clear definition.
Usually, it’s due to rapid blood flow increase from VCI to heart and consequent rise of intracardiac pressure. Myocardial contusion is a common injury in blunt cardiac trauma, and it usually includes trauma of left anterior descending artery. Rare injuries include trauma of valves, tendinous chords, rupture of papillary muscle and blunt pericardial rupture.
Clinical Features of Thoracic Trauma
Knowing that thoracic trauma may present itself in a very wide spectrum of clinical scenarios, and always having in mind that minor-injury appearing patients may be the ones with rapid deterioration and fatal outcome, one must very seriously and carefully evaluate every trauma patient.
Primary estimation is roughly based to exclude Lethal Six, whereas secondary assessment is focused on Hidden Six.
The following steps should be undertaken:
ABC
- Airway (be careful to examine C-spine first) assessment with intubation if required
- Breathing: Inspection, palpation, percussion and auscultation
- Circulation: Blood pressure, gas exchange tests
Secondary survey
- Lung contusion: The presence of multiple rib fractures or a flail chest should warn the emergency doctor about the possibility of a lung contusion. Moreover, a patient with a lung contusion is likely to show difficulties with maintaining a good peripheral oxygen saturation despite optimum oxygen supplementation therapy.
- Cardiac tamponade: Be aware of Beck’s triad: distended neck veins, hypotension, heart sounds muffled < other signs such as a rise in jugular vein pressure on inspiration, paradox pulse and PEA arrest may be present.
- Cardiac contusion: Non-specific clinical presentation ranging from asymptomatic to complaints of chest pain and shock. Overlap with other thoracic injuries is common and should be kept in mind.
- Rib fractures and flail segment: Pain and tachypnea, paradoxical movement in unintubated patients, crepitation on palpation of broken rib ends, as well as moderate to severe respiratory distress in proportion to injury extent.
- Blunt aortic injury: Interscapular murmur on auscultation, low blood pressure.
- Esophageal injury: Pain when swallowing, crepitus in the neck.
- Diaphragmatic rupture: May present as auscultated bowel sounds in the chest or dullness on percussion of the chest.
- Thoracic vertebral fractures: Important not to miss to assess it, could be presented by ‘step’ deformity or spinous process tenderness on palpation in the secondary survey. It’s important to include lateral thoracic spine X-ray or evaluate thoracic spine on CT scan done for general evaluation. The integrity of vertebral bodies and integrity of conceptual columns of the spinal column is evaluated.
Investigations for Thoracic Trauma
Chest X-ray
It’s a simple and fast method that can be used initially in the evaluation of different thoracic structures. It’s used in the evaluation of the chest wall fracture, pneumothorax, hemothorax, lung contusion areas, widening of aortic arch shadow, diaphragmatic contour.
CT scan
A CT scan of the chest is considered the imaging diagnostic tool of choice in the assessment of thoracic injuries as it has high sensitivity and specificity. Different thoracic structures can be evaluated with high accuracy to make decisions in the management of the patient.
It’s used in the examination of bone fractures, small pneumothorax, cardiac, aortic, pulmonary vessel injuries, pneumo and hematomediastinum, diaphragmatic rupture, lung contusions.
Echocardiography
Transthoracic echocardiography (TTE) is a very important diagnostic tool in the assessment of the cardiac injuries as it can show the pericardial effusion and reveal whether the patient is in echocardiographic findings of cardiac tamponading or not.
Echocardiography-guided pericardicentesis is both diagnostic and therapeutic in the case of hemorrhagic pericardial effusion.
Injuries associated with cardiac tamponade include cardiac contusion and coronary artery injury which may have a delayed presentation that presented with ventricular septal rupture (VSR).
Management of Thoracic Trauma
Management of thoracic trauma requires a multidisciplinary team effort. Depending on the severity of the injury, the patient might be treated and discharged home from the emergency department or might need to be admitted to the intensive care unit.
Life threatening conditions are assessed and treated first; therefore, no imaging should delay treatment.
Most frequent injuries are treated as follows:
Tension pneumothorax
Needle decompression is done by insertion of a 14 gauge, 5cm long needle in the second intercostal space in the mid-clavicle line. Once the needle decompression is done, the pleural space is decompressed then it’s time for further diagnosis exams and definitive management, which is the insertion of a formal chest drain.
Open pneumothorax
Immediate management – supplemental (100%) oxygen, flap-valve dressing, insertion of a chest drain and applying of occlusive dressing to the wound.
Hemothorax
100% oxygen, followed by insertion of intercostal chest drain and maintenance of circulating volume.
Cardiac contusion
Urgent intervention may be mandatory and life-saving.
Resuscitation procedure, combined with 100% oxygen and intravenous fluid or blood products administration should increase cardiac input pressure, temporarily buying time and improving the situation. The sole aim of therapy is to maintain cerebral perfusion.
Systolic pressure should not be elevated because it will increase the cardiac rate and potentially the volume of blood in the pericardial sac.
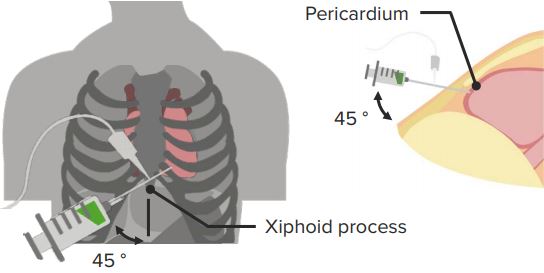
If needed, a needle pericardiocentesis can be performed by insertion of a large bore needle between the xiphisternum and left subcostal margin. Evacuation of even a small amount of blood (such as 50ml) could improve the situation.
If pericardiocentesis fails, urgent surgery and decompression is necessary. When pericardiocentesis is done, a severe danger of damage to coronary vessels is present.
Lung contusion
3 – 5 days supportive period is required to follow up the resolution of contusion, involving supplemental oxygen, and analgesia in order to avoid complications.
Pneumonia is one of the most frequent ones. ARDS and respiratory failure are potential complications of severe contusion.
Simple rib fracture
It is treated by analgesia and targeted physiotherapy in order to prevent complication due to inadequate respirations. Special focus should be on underlying conditions.
Complications of Thoracic Trauma
Common complications of thoracic trauma include:
- Respiratory failure
- Pneumonia
- Pleural sepsis (in cases of retained hemothorax by external contamination of thoracostomy tube)
Complications of management of cardiac trauma include:
- Internal mammary and coronary artery injury
- Ventricular puncture and aspiration
- Introduction of infection and pericarditis
- Phrenic nerve injury during surgical approach through the pericardial sac



{kind=link}
Comentários
Enviar um comentário