Toxic Shock Syndrome (TSS) in Children — Symptoms and Diagnosis
Table of Contents
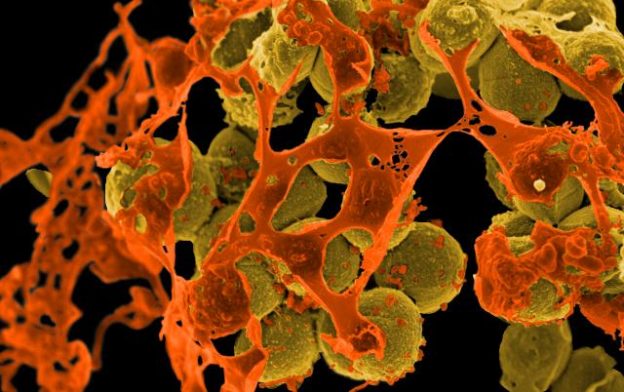
Image: “Scanning electron micrograph of methicillin-resistant Staphylococcus aureus (MRSA, brown) surrounded by cellular debris. MRSA resists treatment with many antibiotics.” by NIAID/NIH. License: Public Domain
Definition
Toxic shock syndrome can be defined as acute illness caused by toxin-producing staphylococcus aureus.
It is a multi-system disease that presents with organ failure in addition to fever, rash, hypotension, and skin manifestations.
Etiology
Toxic shock syndrome is caused by toxin producing strains of staphylococcus aureus and streptococcus.
Epidemiology
One of the most common causes of toxic shock syndrome was the use of tampons in menstruating adolescent girls. Nowadays, the tampons used need to be changed more often so they are less likely to cause staphylococcus aureus bacterial growth and toxic shock syndrome. The current incidence of toxic shock syndrome related to the use of tampons in female adolescents and young adults is approximately 0.5 per 100,000.
50% of cases are from tampons (all staph aureus), especially super-absorbent tampons.
Nowadays, the incidence of toxic shock syndrome related to the use of tampons and those that are not related to tampon usage is almost equal. One particular group of children that is at risk of developing toxic shock syndrome are those that are admitted to the burns unit due to skin burns. Approximately, 10% of these children might end up with toxic shock syndrome.
Toxic shock syndrome was found to be uncommon in children younger than 10 years for obscure reasons. Another common cause of toxic shock syndrome in children is post-operative complication. Approximately, 16 in every 100,000 who undergo an ear, nose or throat surgery will develop toxic shock syndrome.
Children are also at risk of developing streptococcal toxic shock syndrome. Group A streptococcus is responsible for approximately 4 in every 100,000 general population cases of toxic shock syndrome per year. While streptococcal toxic shock syndrome is more common in the elderly, children aged younger than 2 years are at a particular increased risk.
While children might develop streptococcal toxic shock syndrome, the mortality rate is usually lower compared to adults. The mortality rate of streptococcal toxic shock syndrome in children is estimated to be around 5%.
Pathophysiology of Toxic Shock Syndrome in Children
Toxic shock syndrome is most likely an immune mediated disorder that is activated by a superantigen. This superantigen is most likely a toxin produced by certain strains of staphylococcus aureus.
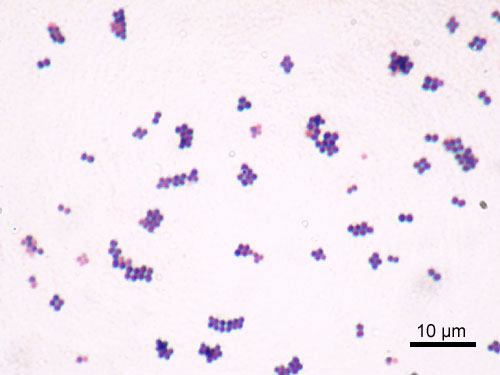
Image: “Microscopic image of Staphylococcus aureus (ATCC 25923). Gram staining, magnification:1,000.” by Y Tambe. License: CC BY-SA 3.0
The most commonly produced toxins responsible for staphylococcal toxic shock syndrome in children are:
- Toxic shock syndrome toxin-1 (TSST-1) which is found in 75% of the patients.
- Enterotoxin-b which is found in approximately 23% of the patients with toxic shock syndrome.
- Enterotoxin-c which is found in only 2% of the patients.
Staphylococcus aureus strains that produce TSST-1 are commonly identified in the vagina and in the nasopharynx of patients presenting with toxic shock syndrome. This explains the clear association between toxic shock syndrome and the use of tampons in menstruating women or ear, nose and throat surgery in non-menstruating children.
Streptococcal superantigens are responsible for the other form of the disease known as streptococcal toxic shock syndrome. Group A invasive streptococcus are more likely to produce these superantigens, hence their association with the development of toxic shock syndrome.
Another important risk factor for the development of toxic shock syndrome in children is the lack of specific antibodies against TSST-1 or streptococcal superantigens. Patients without a proper immune response are more likely to develop recurrent toxic shock syndrome and the disease might be more invasive.
Clinical Presentation of Toxic Shock Syndrome in Children
Fever is usually high grade, > 39° C. chills, myalgia, malaise, headache, sore throat, muscle tenderness, fatigue, and abdominal discomfort, vomiting, diarrhea, altered level of consciousness, confusion and desquamative skin rash are commonly found in staphylococcal toxic shock syndrome.
Patients with streptococcal toxic shock syndrome might have a fever or not. They usually present with severe systolic hypotension, acute respiratory distress syndrome, a generalized desquamative skin rash and localized soft tissue necrosis.
Patients might also develop myositis or necrotizing fasciitis. Renal impairment and coagulopathy, along with an increased risk of bleeding disorders, are commonly seen in patients with toxic shock syndrome due to group A invasive streptococcus.
Recent medical history can also help differentiate between staphylococcal and streptococcal toxic shock syndrome. Patients with staphylococcal toxic shock syndrome might have a recent history of the use of tampons, or skin burns.
On the other hand, patients with streptococcal toxic shock syndrome might develop the condition as a superimposed infection after the eruption of a varicella related rash.
Gastrointestinal symptoms are more common with staphylococcal toxic shock syndrome, whileinflammation of the muscles and an elevated creatinine kinase are more commonly seen in streptococcal toxic shock syndrome.
Multi-organ failure manifests as hypotension, acute renal injury, and abnormal liver function as depicted below.
Diagnostic Workup for Toxic Shock Syndrome in Children
Patients with toxic shock syndrome develop multi-system dysfunction. To diagnose staphylococcal toxic shock syndrome, the patient has to have a fever, a skin rash, hypotensionand desquamation. In addition to that, three of the following signs of multi-system dysfunction are needed to confirm the diagnosis.
Symptoms suggestive of gastrointestinal involvement or severe myalgia in addition to an elevated serum creatinine and serum urea nitrogen levels are suggestive of acute renal injury. Elevated total bilirubin, AST and ALT levels are suggestive of hepatic injury. Thrombocytopeniacan be also found in staphylococcal toxic shock syndrome.
Bacteremia is rare in staphylococcal toxic shock syndrome but, if a blood culture was performed, it may be positive for staphylococcus aureus. Other causes of a similar clinical picture, such as Rocky Mountain spotted fever or measles, should be excluded by serologic tests.
Patients with streptococcal toxic shock syndrome are expected to have a similar semiology but they are more likely to have an elevated creatinine kinase suggestive of myonecrosis.Creatinine levels are usually elevated due to acute kidney injury. Thrombocytopenia and impaired hepatic function is also seen with streptococcal toxic shock syndrome.
A chest X-ray in streptococcal toxic shock syndrome might reveal a characteristic picture of diffuse lung edema and infiltrates typical of acute respiratory distress syndrome. Blood cultures are more likely to be positive with streptococcal toxic shock syndrome compared to staphylococcal because bacteremia is more common with streptococcal etiology.
Treatment of Toxic Shock Syndrome in Children
Patients with toxic shock syndrome should be admitted to the burns unit as they are usually hemodynamically unstable. In addition to adequate fluid replacement therapy, proper antibiotic use is also warranted.
Patients with probable or confirmed staphylococcal toxic shock syndrome should undergo a full examination to identify the most likely origin of the infection. Tampons, if found, should be removed and skin abscesses should be drained.
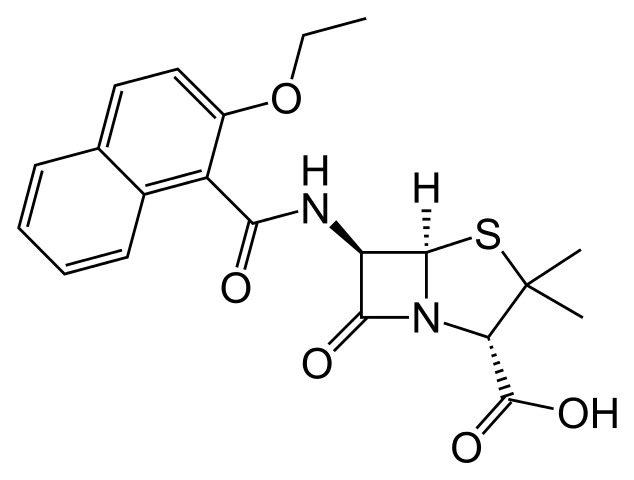
Image: “Structural diagram of nafcillin.” by Fvasconcellos – Own work. License: Public Domain
Antibiotic use is then indicated. Nafcillin, oxacillin or a first generation cephalosporin are first-line therapies for staphylococcus aureus infections. If the patient is found to have a methicillin-resistant strain of staphylococcus aureus, he or she should be switched to vancomycin.
The problem with nafcillin, oxacillin and cephalosporins is that they are more likely to cause an acute increase of the release of TSST-1 once initiated. Because of this, clindamycin, erythromycin or rifampin have been suggested to be used as first-line therapies for staphylococcal toxic shock syndrome.
Streptococcal toxic shock syndrome should be treated with clindamycin. Recent studies suggest the combination of clindamycin with penicillin for optimum results with streptococcal toxic shock syndrome. Unfortunately, mortality remains higher with streptococcal toxic shock syndrome compared to staphylococcal toxic shock syndrome.
Patients with severe shock might benefit from receiving intravenous immunoglobulins in addition to antibiotic therapy as intravenous immunoglobulins can be effective when used in the case of superantigens.
Complications
Complications of toxic shock syndrome include:
- Renal failure.
- Gangrenous/cyanotic extremities.
- Neuropsychiatric manifestations, such as memory loss and lack of concentration.
- Acute respiratory distress syndrome (ARDS) in 55% of patients, especially in streptococcal type.
- Death in 30% of patients



_Bacteria.jpg){kind=link}
{kind=link}
{kind=link}
Comentários
Enviar um comentário