Pregnancy Nutrition
Table of Contents
Nutrition in Pregnancy
Many women have a successful pregnancy without meeting the recommended energy intake guides. This is because different adaptive strategies can be used to cater for the increased energy demands during pregnancy such as:
- By reducing the exertion, energy demands can be lowered
- By increasing absorption of nutrients
- Reduced BMR
- Reduced diet-induced thermogenesis
- Use of already stored fat
These strategies may help in the presence of sub-optimal nutritional status but there is a physiologic limit to adjust nutrient metabolism, and hence the growth and development of the fetus may be affected. In the case of an under-nourished woman, nutrient supply is physiologically driven more to the mother and the fetal growth is compromised to a greater extent.
Weight loss is not at all recommended by dieting during pregnancy even if mother is morbidly obese. Medicines for weight management should be avoided during time of conception and pregnancy.
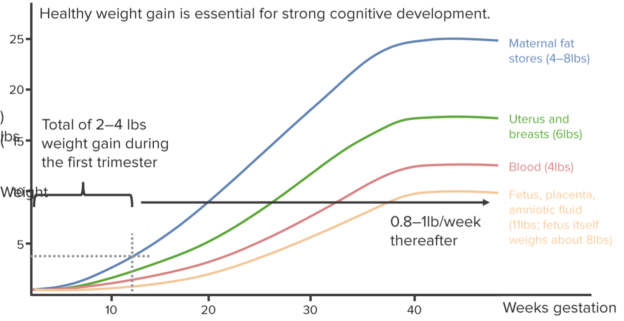
There are no increased energy demands in the first trimester. 340 kcal extra energy is required in the second trimester, and an additional energy of 452 kcal is the need of the third trimester. However, there are significant variations in the energy requirements based on weight before pregnancy and individual body height.
Weight gain during pregnancy is due to the combination of the following:
- Water (about 62 %)
- Fat mass (about 30 %)
- Protein (about 8 %)
Adequate plasma volume expansion is directly related to a favorable pregnancy outcome.
Recommended total weight gain in pregnant women based on pre-pregnancy BMI (kg/m2)
For multiple births, need for nutrients and calories for pregnant women is higher than those who have single fetus in the womb with the requirement of 40-45 kcal per day.
Protein
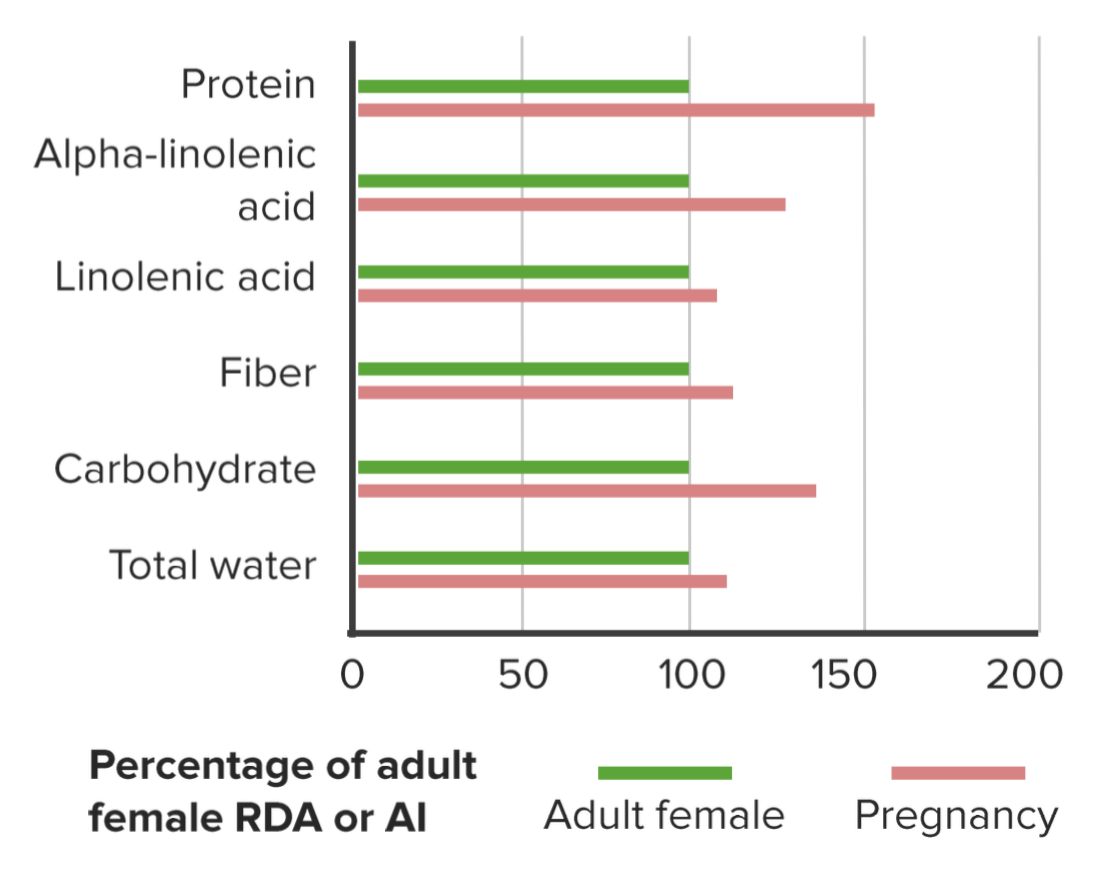
There is a higher demand for proteins during pregnancy to support the weight gain and fetal growth, specifically in the last trimester. Metabolic adaptation increases the efficiency of protein synthesis during pregnancy.
Recommended protein intakes for pregnant women
No additional protein requirement are there in the first trimester of pregnancy. Therefore the RDI for protein in women aged 19-50 in the first trimester is 0.75 g per kg per day.
The RDI for protein in women aged 19-50 in the second and third trimester is 1.0 g per kg per day and for women 14-18 years old, it is 1.02 g per kg per day.
The sources of protein are milk, eggs, meat, chicken, cheese, and lentils.
Carbohydrates
Carbohydrate metabolism is constantly altered throughout the pregnancy to ensure that the fetus receives an adequate supply of macronutrients even if the maternal nutrition is intermittent. Adequate glucose is required for maternal brain metabolism and as a primary energy resource for the fetus.
45–65 % of total energy comes from carbohydrate for adults over 14 years of age. During pregnancy, the recommended dietary allowance for carbohydrate intake in is 175 g per day. This is 45 g more than the carbohydrate requirement of non-pregnant females.
Dietary Fiber
Due to high levels of progesterone, there is a decreased GI transit during pregnancy. This is beneficial in a sense that food is in contact with the absorption sites for a longer period, hence improved absorption but it also leads to constipation.
Therefore, adequate intake of dietary fiber is necessary to maintain regular bowel habits during pregnancy. The recommended dietary allowance for pregnant women aged 19–50 years for dietary fiber intake is 22 g per day. To meet the recommended daily needs for both carbohydrates and fiber, low energy density food or low GI food sources should be taken such as fruits, cereals, whole grain and vegetables.
Fats
Fatty acids fulfill half of the energy needs of the fetus during early pregnancy. In the later stages, the fetus forms its own fatty acids. Long-chain polyunsaturated fatty acids are essential for brain growth and development in infants, specifically in the third trimester, when the growth of nerve tissue is at its highest.
The fetus has a limited ability to synthesize long-chain polyunsaturated fatty acids and therefore is dependent upon the placental supply. Obese women who have insulin resistance and those who are thin with little body fat, are more in need of dietary fat to maintain the adequate supply to the fetus. Recommended doses for essential fatty acids and omega 3 long-chain polyunsaturated fatty acids for pregnant women aged 19–50 years are as follows:
- Linoleic acid: 10 g per day
- Alpha-linolenic acid: 1 g per day
- Total omega-3 long-chain polyunsaturated fatty acids: 115 mg per day
Minerals
Iron
Iron deficiency is the most common deficiency in pregnant women. It leads to impaired red blood cell function and anemia, which in turn increases the risk of post-partum infections, hemorrhage, heart failures and mortality.
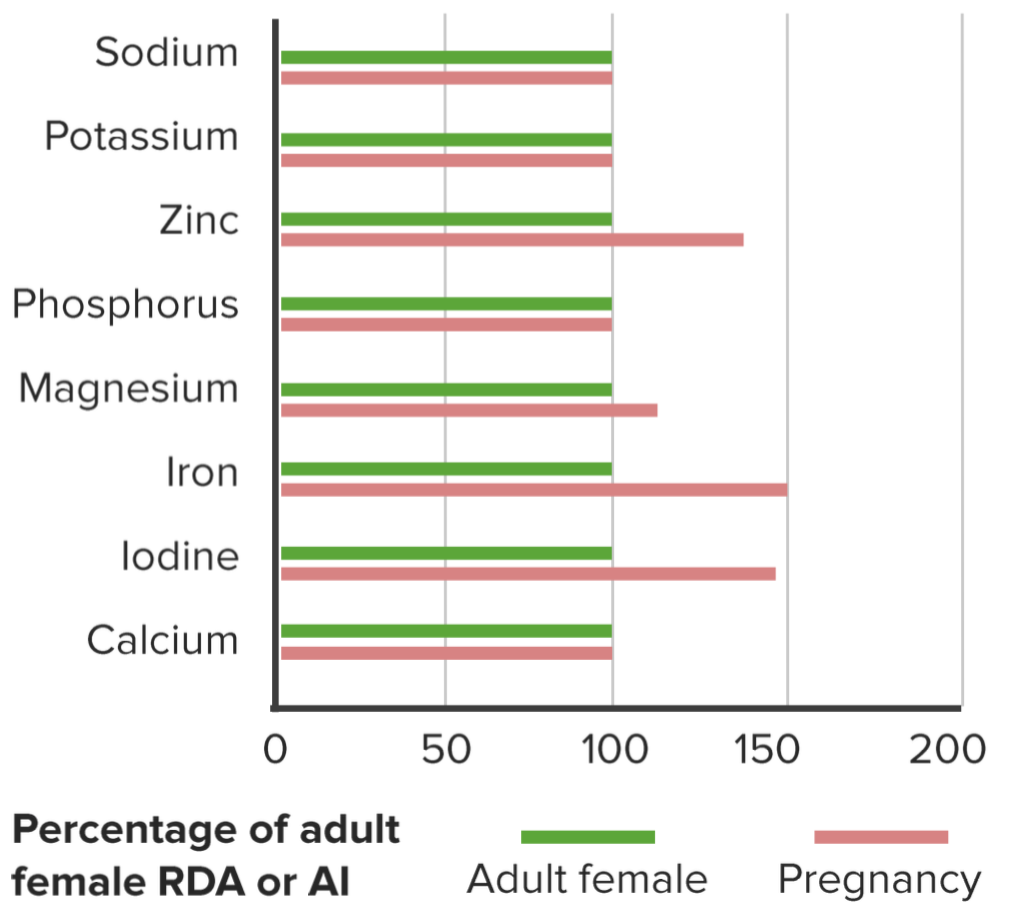
The recommended dose for pregnant women of ages 14–50 is 27 mg per day. Iron requirements during the first trimester are less than the others, but these doses are recommended to build the iron stores for the last trimester of pregnancy.
The sources of iron in diet are dried beans, animal protein, fortified food and any food that is cooked in the iron utensils.
Calcium
There is increased demand for calcium during pregnancy but this need is largely fulfilled by greater maternal calcium absorption, retention, and turnover in the first trimester. Its demand is high because of continuous building of fetal tissue , especially in third trimester. The recommended allowance for pregnant women aged 19–50 is 1,000 mg per day. It is the same as that for non-pregnant and non-breastfeeding women.
The dairy products and green leafy vegetables are highly rich in calcium needed for Vitamin D absorption and are recommended for pregnant ladies.
Zinc
Any deficiency in zinc during pregnancy can result in neural tube defects, premature delivery, low birth weight and other complications. The recommended allowance for pregnant women aged 14–18 is 10 mg per day, and for women aged 19–50, it is 11 mg per day.
A well balanced diet meet the requirement of the zinc for the pregnant ladies, extra supplementation is not recommended when iron supplements cross 60 mg per day.
Selenium
Increased demands of selenium during pregnancy account for the promotion of fetal growthand selenoprotein synthesis. The recommended allowance for pregnant women aged 14–50 is 65 μg per day.
Magnesium
Deficiency of magnesium results in uterine hyper-irritability, fetal growth retardation, cerebral palsy and pregnancy-induced hypertension. The recommended allowance for pregnant women aged 14–18 is 350 mg per day, for women aged 19–30, it is 360 mg per day, and women aged 31–50, it is 360 mg per day.
Iodine
High rates of growth in fetus increases the maternal needs for iodine. Deficiency of iodine can result in abortion, stillbirths, birth defects and neurological defects. The most vulnerable group in case of iodine deficiency is the pregnant women. The recommended allowance for pregnant women aged 14–50 is 220 μg per day and iodized salt can prevent iodine deficiency.
Copper
There is copper accumulation in the fetus, amniotic fluid, and newly formed maternal tissue. This increases the copper demand during pregnancy. The recommended allowance for pregnant women aged 14–50 is 1.3 mg per day.
Sodium
To maintain the increased plasma volume during pregnancy, sodium requirements are more than normal. Acceptable intake for pregnant women aged 14–50 is 460–920 mg per day.
Potassium
There is an overall small increase in potassium needs during pregnancy, but this does not require supplemental intake. Hence the adequate intake is the same as for non-pregnant women, i.e., 2,800 mg per day.
Sulphate
The higher sulphate requirements during pregnancy can be met from water and protein rich diet that has sulphur containing amino acids.
Fluoride
It is necessary for the developing deciduous teeth of the fetus. There are no increased fluoride requirements during pregnancy. The recommended allowance is 3 mg per day.
Vitamins
Vitamin A
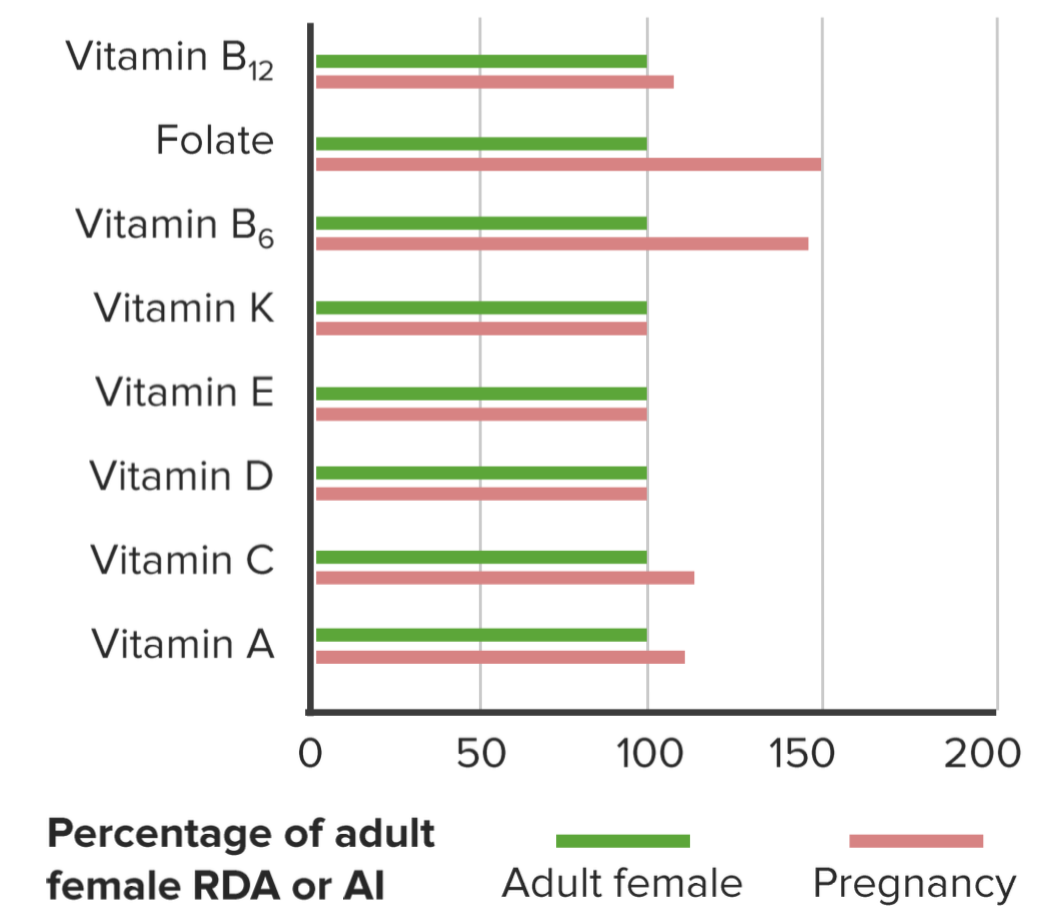
Sufficient supplies of vitamin A play their role in birth weight, circumference and length of head, and the duration of gestation. It helps in glycoprotein synthesis and cellular growth. Sub-optimal levels are associated with increased maternal motility. The recommended allowance for pregnant women aged 19–50 is 800 μg REs per day. There is only 10 percent increase in the daily requirements, greater than this can be harmful to the fetus.
The source of Vitamin A are green leafy vegetables and orange vegetables.
Vitamin D
Deficiency of vitamin D during pregnancy results in decreased fetal growth. This is due to the effect of vitamin D deficiency on maternal calcium homeostasis. The recommended dose for pregnant women aged 19–50 is 5 μg of vitamin D per day.The source of Vitamin D is fortified milk.
Vitamin E
The recommended dose for pregnant women aged 19–50 is 7 mg per day. It is the same as that for non-pregnant women. It can be extracted from animal fats and proteins.
Vitamin K
The recommended dose for pregnant women aged 14–50 is 60 μg per day. It is the same as that for non-pregnant women. Its rich sources are green leafy vegetables, eggs, tomatoes, and dairy products.
Folate
The decrease in serum and red cell folate levels is teratogenic in early pregnancy. Any deficiency leads to neural tube defects, megaloblastic anemia of pregnancy, atherosclerosisin mother and cervical dysplasia. The recommended dose for pregnant women aged 14–18 is 800 μg per day and dose for pregnant women aged 19–50, it is 1,000 μg per day.
Thiamin (vitamin B1)
The deficiency of vitamin B1 during pregnancy affects the growth of the fetus and increases the risk of congenital malformations such as cleft lip and palate, sudden infant death syndrome, and pre-eclampsia. The recommended dose for pregnant women aged 14–50 is 1.4 mg of vitamin B1 per day.
Riboflavin
Deficiency of riboflavin can cause pre-eclampsia. The recommended dose for pregnant women aged 14–50 is 1.6 mg of riboflavin per day.
Riboflavin is found in green vegetables, eggs, cheese, milk and fish. Routine intake of riboflavin is not recommended.
Niacin
The increased demands for niacin during pregnancy are related to the increased energy requirements and growth of the fetus. The recommended dose for pregnant women aged 14–50 is 18 mg niacin per day.
Pantothenic acid
The recommended dose for pregnant women aged 14–50 is 5 mg per day. It is the same as that of non-pregnant women.
Vitamin B6 (pyridoxine)
It is essential for the nervous system development, and any deficiency will affect the brain of the fetus. It is essential for the metabolism of protein, carbohydrate and lipid. The recommended dose for pregnant women aged 14–50 is 1.9 mg of vitamin B6 per day.
Vitamin B12 (cobalamin)
It is essential for normal hematological and neurological functions. The recommended dose for pregnant women aged 14–50 is 2.6 μg per day. It is found in proteins extracted from animals.
Biotin
It is essential for fetal development, and the fetus depends on maternal dietary intake. The recommended dose for pregnant women aged 14–50 is 30 μg per day. This amount is 5 μg more than that required for non-pregnant women.
Its rich sources are fortified grains, green leafy vegetables and dried beans.
Vitamin C
Any deficiency in vitamin C during pregnancy is associated with ruptured placental membranes, infections and premature births. The recommended dose for pregnant women aged 14–18 is 55 mg per day. The dose for pregnant females aged 19–50 is 60 mg per day.
The sources of Vitamin C are fruits and vegetables without routine supplementation as balanced diet can meet the requirements of vitamin C.
Water
The need for water intake during pregnancy is 3.1 liters per day in total. About 2.3 liters of this need is fulfilled by drinking water and the rest through food and other fluids.
Prenatal Nutrition: Breastfeeding or Formulas?
Breastfeeding is recommended as the best option for the newborn. It should be exclusively practiced for 6 months and is recommended for up to 12 months. Breast milk prevents allergies and helps improve immunity. A formula is a healthy option in the absence of breastfeeding.



Comentários
Enviar um comentário