Traumatic Brain Injury (Craniocerebral Trauma; TBI) — Symptoms and Treatment
Table of Contents
- Overview
- Minor Head Injuries
- Etiology
- Glasgow Coma Scale and the Severity of Head Injury
- Classification of traumatic brain injuries
- Major Head Injuries
- Computed Tomography Scan Findings in Traumatic Brain Injuries
- The Possibility of a Significant Intracranial Injury in Patients with a Mild Traumatic Brain Injury
- References
Overview
Major head injuries are managed very differently from non-serious head injuries. A major head injury is defined as any traumatic brain injury with severe disturbance of consciousness and/or focal neurological deficits. A minor head injury, on the other hand, is defined as a traumatic brain injury with no loss of consciousness, or loss of consciousness for a duration that is less than 10 minutes.
Minor Head Injuries
Patients with a minor head injury might sustain a cerebral injury. Such patients can be classified into those who lost consciousness for any period of time that is limited to 10 minutes and those who did not lose consciousness. Patients who did not lose consciousness at all and are determined to have a minor head injury can be sent home. Such patients typically have a Glasgow Coma Score of 15 out of 15.
Patients discharged home with the diagnosis of mild traumatic brain injury should be instructed to look for signs of neurological deterioration.
Etiology
Head injuries may arise from:
- Motor vehicle accidents
- Fall from a height
- Contact sports-related injuries
- Penetrating trauma
Indications for immediate re-visit to the emergency department are:
- Severe refractory headache
- Repeated vomiting
- Development of seizures
- Alteration in the level of consciousness
Patients diagnosed with a mild traumatic brain injury who have lost consciousness for a period of time that is below 10 minutes as per the definition should be examined more carefully, and the possibility of a significant cerebral injury should be excluded. Patients with severe headaches, confusion, or seizures who present to the emergency department with a mild traumatic brain injury should receive a computed tomography scan of the brain to exclude cerebral injury.
Moreover, patients bleeding from the nose or ear who are determined to have a minor head injury should be evaluated for the possibility of a basal skull fracture. Patients with mild traumatic brain injury and large lacerations or hematomas of the scalp are more likely to have a fracture of the skull.
Patients with minor head injuries due to a localized force to the head might develop a depressed fracture. If the physical examination reveals a soft hematoma with depression, the possibility of a depressed fracture is quite high.
Glasgow Coma Scale and the Severity of Head Injury
The following table summarizes the Glasgow Coma Scale (GCS) which is a score that is indicative of the degree of consciousness in head trauma patients:
As it is obvious, the GCS can range between 3 and 15 out of 15. Some studies showed that the motor component of the GCS is better correlated with physical independence in the long-term post traumatic brain injury compared to the total GCS. The GCS should be determined only after the patient is fully resuscitated for the purposes of classification of the severity of the traumatic brain injury.
Classification of traumatic brain injuries
Classification can be done using various methods, such as:
- Severity classification
- Anatomical classification
- Pathological classification
- Primary versus secondary brain injury
The classification according to severity classifies patients with traumatic brain injury according to GCS scores into:
- Mild head injury with a GCS of 14 to 15/15 at the time of presentation to the emergency department.
- Those with a GCS of 9 to 13/15 are considered as having a moderate traumatic brain injury.
- Patients with a GCS of 8 or less are diagnosed with severe traumatic brain injury.
Patients with a GCS of 14 at the time of presentation should receive another GCS assessment two hours after their trauma. If the GCS is still below 15, they should be considered for a brain computed tomography scan. If the GCS falls two points or more at any given time, a brain computed tomography scan should be performed immediately.
Major Head Injuries
A major head injury is defined as any head injury that results in a GCS of 8 or less at the time of presentation. Patients with moderate traumatic brain injuries can also be classified as serious head injuries. Patients with symptoms and signs suggestive of a significant intracranial injury, who have a mild traumatic brain injury per their GCS, can also be considered as having a serious head injury.
Patients with severe traumatic brain injuries should receive a computed tomography scan of the brain to exclude intracranial pathologies, including hemorrhage and fractures.
Computed Tomography Scan Findings in Traumatic Brain Injuries
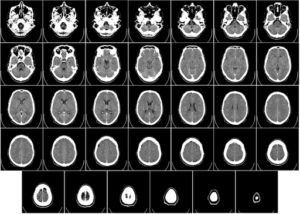
A computed tomography scan of the head is indicated to exclude a significant cerebral injury, rather than to confirm the diagnosis of skull fracture. If, however, a fracture is seen on the computed tomography scan, such a finding should be documented.
Intracranial Hemorrhage in a Traumatic Brain Injury
Epidural hematoma
An epidural hematoma, also known as an extradural hematoma, is seen on the computed tomography scan as a hyperdense convex shape. It can be ipsilateral to the site of trauma, or can be found on the contralateral side, i.e. in coup-contracoup injuries. The size of an epidural hematoma can be determined with the following formula: 0.5 x height in cm x length in cm x depth in cm.
Subdural hematoma
A subdural hematoma is more commonly seen in the elderly, or in patients with brain atrophy. This can be explained by the understanding of the pathophysiology of subdural hematomas. For subdural hematoma to occur, one expects the brain to shake within its space and such a force to cause rupture of the small venules that bridge between the dura and the brain.
A young patient with no brain atrophy is, therefore, less likely to develop a subdural hematoma compared to an older patient with brain atrophy. Subdural hematoma might be acute (hyperdense), subacute (isodense), or chronic (hypodense). The shape of a subdural hematoma is concave.
Subarachnoid hemorrhage
Rarely presents with features suggestive of trauma, but more of increased intracranial pressures.
Intracerebral hematoma and cerebral contusions present as hyperdensities within the brain parenchyma.
Intracranial hemorrhage predisposes the patient to an increased risk of early post-traumatic seizures; therefore, antiepileptic prophylaxis, typically with phenytoin, is indicated. Antiepileptic prophylaxis is usually used for 7 days.
Patients with intracranial hemorrhage might develop significant elevations in the intracranial pressure. An elevation in the intracranial pressure is associated with impaired cerebral perfusion, ischemic brain injury, and cytotoxic cerebral edema. Osmotic therapy, diuresis, hyperventilation, and, in some cases, surgical decompressive craniectomy are the main treatments for raised intracranial pressure post-traumatic brain injury.
Patients with large epidural or subdural hematomas and signs suggestive of an elevated intracranial pressure should undergo burr-hole evacuation of the epidural hematoma or craniotomy to evacuate the subdural hematoma.
Fractures of the Skull
In contrast to skull X-rays, computed tomography scans of the head have good sensitivity for the detection of skull linear fractures, depressed fractures, and basal skull fractures.
Classification of skull fractures
They can be simple fractures that have no communication with the atmosphere and could be linear, comminuted, cracked or ping-pong in nature or compound fractures that communicate with the atmosphere.
Patients with symptoms and signs suggestive of a basal skull fracture, such as raccoon eyes, battle sign, or rhinorrhea, should receive a head computed tomography scan with 2 or 3 mm thick slices to confirm the diagnosis of the basal skull fracture.
The presence of a linear fracture on the head computed tomography scan is an indication for hospital admission for 24 hours in some hospitals. This is related to the fact that an epidural hematoma is more likely to develop when there is a linear fracture of the skull compared to when the patient does not have any fractures, especially within the first 24 hours after the trauma.
The Possibility of a Significant Intracranial Injury in Patients with a Mild Traumatic Brain Injury
The following characteristics raise the possibility of a significant intracranial injury in patients with a mild traumatic brain injury:
- A GCS below 15 at 2 hours post-injury
- Deterioration in GCS by two points
- Focal neurological deficits
- Clinical suspicion of a basal skull fracture
- Recurrent vomiting, more than 3 times, at the emergency department
- History of coagulopathy, bleeding disorders, or use of anticoagulation therapy
- Age above 65 years
- Post-traumatic seizures
- Loss of consciousness for more than 5 minutes, but less than 10 minutes post-injury
- Confusion
- Persistent severe headache
- Dangerous mechanism of injury
- Or the patient returned to you after being discharged home with concussion instructions
Patients in this sub-group should receive a computed tomography scan of the brain to reliably exclude the possibility of cerebral injury.



{kind=link}
{kind=link}
Comentários
Enviar um comentário