Gastrointestinal Circulation (Blood Supply of the GI Tract) — Superior Mesenteric Artery (SMA) and Inferior Mesenteric Artery (IMA)
Table of Contents
Image : “A 3D illustration of the abdominal aorta at the iliac junction” by Gegu0284. License: CC BY-SA 4.0
Embryology of the GI Tract
The adult gastrointestinal tract (GIT) is derived embryologically from the primitive gut that is formed from the endoderm lining the yolk sac. The primitive gut is divided into foregut, midgut, and hindgut.
The foregut gives rise to esophagus, stomach, first and second part of duodenum, as well as liver, gallbladder and the superior part of the pancreas. All the organs derived from the foregut are supplied by the branches of the celiac trunk (artery).
The midgut gives rise to distal (third part of) duodenum, jejunum, ileum, cecum, appendix, ascending colon and the proximal two-thirds of the transverse colon. These are supplied by the branches of the artery of the midgut, the superior mesenteric artery.
The hindgut gives rise to distal one-third of the transverse colon, descending colon, rectum and upper part of the anal canal. These structures are supplied by the branches of the artery of the hindgut, the inferior mesenteric artery.
All three unpaired arteries i.e. celiac trunk, superior and inferior mesenteric arteries are branches of the abdominal aorta.
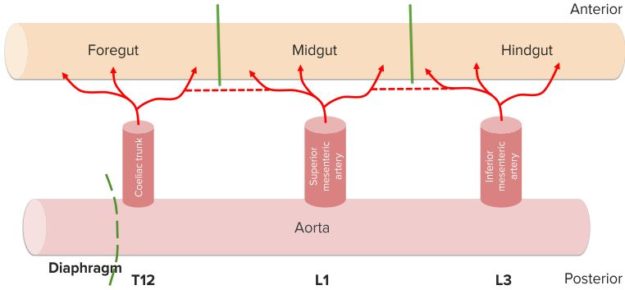
“Blood supply to GI tract. Schematic” Image created by Lecturio
Abdominal Aorta
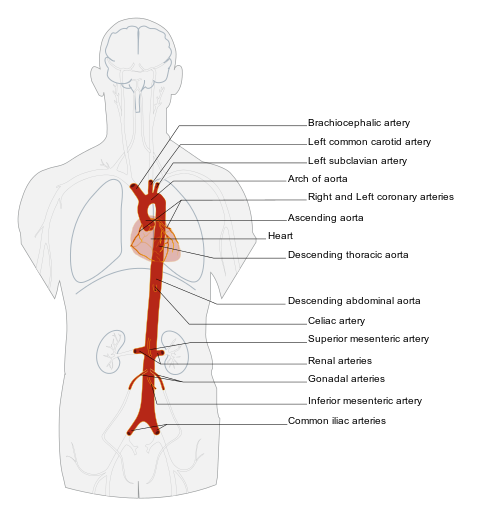
Image: “Aorta artery and it’s branches in anterior view.” by Edoarado – Own work based on: Arterial System en.svg, Coronary arteries.svg. License: CC BY-SA 3.0
The abdominal aorta begins as a continuation of the thoracic aorta at the aortic hiatus of the diaphragm at the level of the T12 vertebra. It ends by bifurcating into the common iliac arteries at the level of the L4 lumbar vertebra.
The GIT is supplied by the three anterior branches of the abdominal aorta. From superior to inferior, their names are the celiac trunk, the superior mesenteric artery and the inferior mesenteric artery. These three branches are individual entities and their terminal branches anastomose to provide the collateral supply.
Celiac Trunk
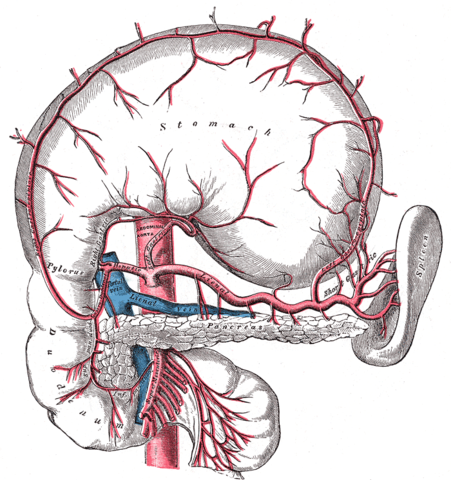
Image: “The celiac artery and its branches; the stomach has been raised and the peritoneum removed.” by Henry Vandyke Carter, Henry Gray (1918) “Anatomy of the Human Body”. Bartleby.com: Gray’s Anatomy, Plate 533. License: Public Domain
The celiac trunk originates from the abdominal aorta and lies in the transpyloric plane at the level of the body of T12 vertebra.
The celiac artery gives three branches that are left gastric artery, splenic artery, and common hepatic artery.
The left gastric artery runs along and supplies the lesser curvature of the stomach.
The splenic artery supplies spleen and pancreas. It gives multiple branches including left gastroepiploic artery that runs along the greater curvature of stomach.
The common hepatic artery divides into the hepatic artery (supplying the hepatobiliary system), right gastric artery (runs along the lesser curvature of stomach) and gastroduodenal artery.
The celiac trunk and its branches supply arterial blood to all the foregut derivatives that include abdominal part of esophagus, stomach, first and second part of duodenum, liver, gallbladder, spleen and superior part of the pancreas.
The celiac ganglia are present on each side of the celiac artery and send sympathetic nerves that travel along with the celiac artery and its branches.
Table 1: Branches of the celiac trunk
Superior Mesenteric Artery (SMA)
This midgut artery originates from the abdominal aorta at the level of the L1 vertebra below the celiac trunk. It then runs antero-inferiorly behind the splenic vein and the neck of the pancreas. During this part of its journey, it is separated from the aorta by the following structures:
- Third part of the duodenum and part of the small intestines, which may be compressed between the SMA and abdominal aorta, causing the superior mesenteric artery syndrome.
- Pancreatic uncinate process, which hooks around the SMA.
- Left renal vein, which can be compressed between the SMA and the abdominal aorta, causing the nutcracker syndrome.
The SMA branches into the intestinal arteries, the inferior pancreaticoduodenal artery, the ileocolic artery and the right and the middle colic arteries. These supply the organs of the midgut, namely the third part of the duodenum, jejunum, ileum, cecum, appendix, ascending colon and proximal two-thirds of the transverse colon.
Inferior Mesenteric Artery (IMA)
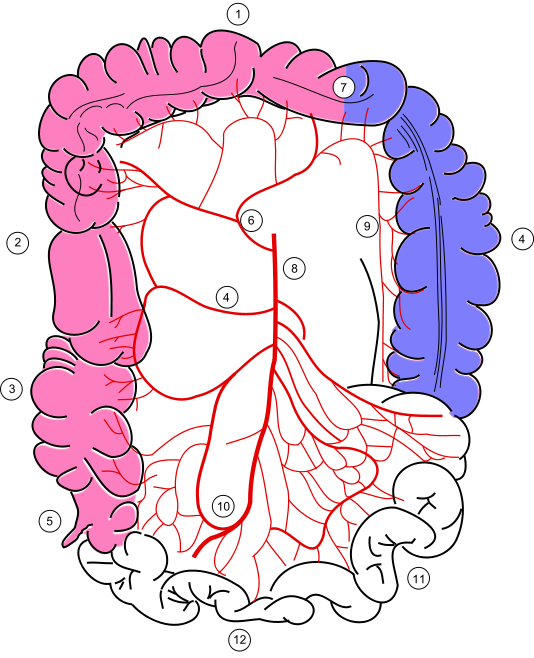
Image: “Colonic blood supply. 1 – transverse colon, 2 – ascending colon, 3 – caecum, 4 – right colic artery, 5 – appendix, 6 – middle colic artery, 7 – Cannon-Böhm point (the border between the areas of SMA and IMA supplies) , 8 – superior mesenteric artery, 9 – marginal artery, 10 – ileocolic artery, 11 – jejunum (partial), 12 – ileum (partial). Proximal small intestine, abdominal organs (pancreas, liver etc), sigmoid and rectum, aorta and inferior mesenteric artery are not shown. Pink – supply from superior mesenteric artery (SMA) and its branches: middle colic, right colic, ileocolic arteries. Blue – supply from inferior mesenteric artery (IMA) and its branches: left colic, sigmoid, superior rectal artery.” by Filip em – Own work based on PD image from Gray’s Anatomy (Image:Gray534.png). Other sources: Schumacher Topographische Anatomie des Menschen (Polish transl., Volumed 1994); Moore & Agur, Essential Clinical Anatomy, 3rd Ed 2007. This vector image was created with Inkscape. License: CC BY 3.0
This hindgut artery arises from the abdominal aorta at the level of the L3 vertebra, inferior to the superior mesenteric artery. It is the smallest branch among the three anterior branches of the abdominal aorta.
Initially, it descends anterior to the abdominal aorta, and then crosses to the left as it continues to descend. It gives off the following branches: left colic artery, sigmoid arteries and the terminal branch, superior rectal arterywhich is a terminal branch. These supply oxygenated blood to the distal one-third of the transverse colon, descending colon, rectum and superior part of the anal canal.
Branches of the SMA and IMA anastomose to form the marginal arteries of Drummond and the Riolan’s arcade(anastomoses between the left colic and medial colic artery). Thus, they provide abundant oxygenated blood to the colon, except for certain watershed areas with poor blood supply, e.g., splenic flexure of the colon.
The marginal artery runs distal, while the arc of Riolan (also known as the meandering mesenteric artery) runs proximal to the root of the mesentery. The terminal branches of the right colic, middle colic, left colic and sigmoid branches enter the colonic wall and are called the vasa recta.
Clinical Relevance of the Abdominal Arteries
Celiac artery compression syndrome
The celiac artery compression syndrome, also called celiac axis syndrome, median arcuate ligament syndrome, and Dunbar syndrome, is a condition characterized by chronic recurrent abdominal pain associated with meals, weight loss, and abdominal bruit. It is a result of the external compression of the celiac artery by the median arcuate ligament.
The diagnosis can be confirmed with imaging such as ultrasound, CT angiography or MRA. Treatment is the surgical excision of the constricting median arcuate ligament to decompress the celiac artery.
Superior mesenteric artery syndrome
This rare syndrome is caused by the compression of the distal third of duodenum between superior mesenteric artery and abdominal aorta. It has to be differentiated from celiac artery compression syndrome as well as nutcracker syndrome.
It is characterized by severe, stabbing, post-meal, abdominal pain, early satiety, nausea, and vomiting. Early diagnosis is difficult but essential as delay can lead to severe dehydration, malnutrition, electrolyte abnormalities, etc. Treatment consists of medical management and, in severe cases, surgical bypass.
Nutcracker syndrome
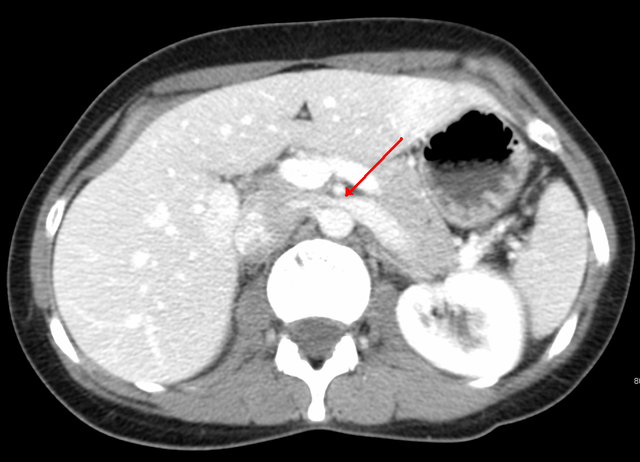
Image: “Compression of the left renal vein (marked by the arrow) between the superior mesenteric artery and the aorta due to nutcracker syndrome.” by James Heilman, MD – Own work. License: CC BY-SA 3.0
This syndrome is characterized by hematuria and left flank pain due to compression of the left renal vein between the abdominal aorta and the SMA.
In the sagittal or transverse plane, the abdominal aorta and the SMA appear like a nutcracker with a nut (the left renal vein) in its jaws, hence the name. The diagnosis of the syndrome is usually confirmed with left renal venography. Treatment consists ofendovascular stenting/renal vein re-implantationdepending on the severity of the symptoms.
Superior mesenteric artery thrombosis
The SMA is rarely affected by atherosclerosis. However, in rare cases, especially following atrial fibrillation or myocardial infarction, the artery may get occluded by a thrombus leading toischemic colitis.
It is characterized by an acute onset of abdominal pain and blood in the stools. In most cases, there is a history of recent myocardial infarction or atrial fibrillation. The watershed area like the splenic flexure is commonly affected. Diagnosis is confirmed with mesenteric angiographyand definitive treatment consists of emergency laparotomy with bowel resection–anastomoses.
Chronic ischemic colitis
When blood flow to parts of the colon is chronically reduced due to arterial blocks or thrombus, the colon may become inflamed and eventually gangrenous. In such situations, we may find the marginal artery and the arc of Riolan significantly enlarged in an attempt to perfuse the ischemic colonic segment.
Left hemicolectomy
This surgical procedure involves the removal of the left side of the large bowel, usually necessary in case of tumors. The IMA and its branches have to be resected during this surgery as the IMA supplies the left colon.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comentários
Enviar um comentário