Bacterial Meningitis in Children — Symptoms and Treatment
Table of Contents
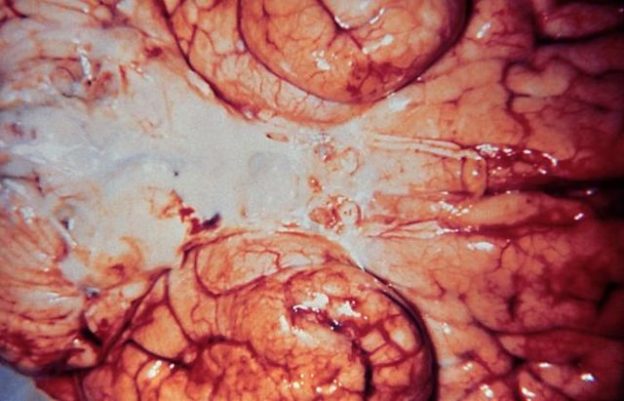
Image: “Inferior view of a brain infected with Gram-negative Haemophilus influenzae bacteria.” Photo Credit: Content Providers(s): CDC – This media comes from the Centers for Disease Control and Prevention’s Public Health Image Library (PHIL), with identification number #5003. License: Public Domain
Definition and Epidemiology of Bacterial Meningitis in Children
Meningitis is a term that means inflammation of the meninges, which include the pia and arachnoid matter. Bacterial meningitis means that the etiology of this inflammation must be a bacterial agent, or at least a bacterial toxin or other kinds of bacterial products.
Image: “Streptococcus Pneumoniae” by Dr. Richard Facklam. License: Public Domain
Nowadays, one of the most important risk factors for meningitis is the absence of preformed antibodies against one of the common etiologies, such as Streptococcus pneumoniae or Haemophilus influenzae due to the lack of vaccination.
Since the introduction of vaccination against the different strains of Streptococcus pneumoniae and Haemophilus influenzae, the risk of bacterial meningitis and the severity of the condition have declined markedly.
Newborns are at highest risk of mortality and morbidity related to bacterial meningitis. The mortality of bacterial meningitis if untreated can be as high as 100 %. Neurological sequelae are also common, even with treatment.
Because of the severity of the complications, and the high mortality rate of bacterial meningitis, early diagnosis and immediate initiation of appropriate antibiotic therapy is essential for optimum survival.
Pathophysiology of Bacterial Meningitis in Children
Most cases of bacterial meningitis are caused by Streptococcus pneumoniae, Haemophilus influenzae and Neisseria meningitidis. Gram negative organisms, such as E. coli, can also cause meningitis in humans, but this is relatively rare compared to other organisms previously mentioned. Bacterial meningitis can also be caused by Listeria monocytogenes or group b streptococci; both of them more common in newborns and young infants.
For the organisms to cause meningitis, they should reach the cranial cavity via various transmission mechanisms such as direct contiguous spread, hematogenous spread and retrograde transmission via nerves.The organisms will then cross the blood-brain-barrier to reach the meninges. The blood-brain-barrier is a physiologic and structural barrier in the brain that limits the access of different agents and toxins, while allowing the entry of certain nutrients. Transcellular traversal of the blood-brain-barrier is the most common mechanism of bacterial entry to cause meningitis.
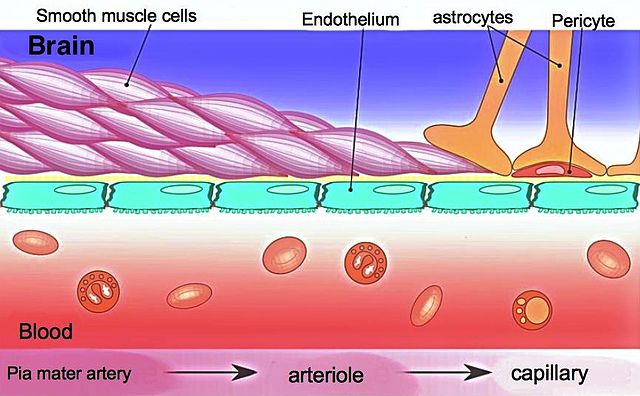
In order for the bacteria to cross the blood-brain-barrier, they need to interact with specific cellular receptors in the barrier to gain access. For instance, the endoplasmin receptor in the blood-brain-barrier has been associated with the pathogenesis of E. coli and Listeria monocytogenesas these two organisms can bind to this receptor.
On the other hand, laminin receptor protein and platelet-activating factor receptors are implicated with Streptococcus pneumoniae, Neisseria meningitidis and Haemophilus influenzae pathogenesis pathway of transcellular traverse of the blood-brain-barrier.
Once the bacteria gain access to deeper structures in the central nervous system, they can infect the meninges and result in an inflammatory response. The release of chemokines and cytokines is responsible for most of the symptoms of the condition, while direct involvement of the brain can result in meningoencephalitis.
Clinical Presentation of Bacterial Meningitis in Children
The child’s age is an important factor in the presence or absence of certain symptoms of meningitis. Infants who develop bacterial meningitis can present with fever, hypothermia, lethargy, poor feeding, vomiting and diarrhea. A bulging fontanelle in patients with open skull fontanelles is a sign of increased intracranial pressure, which can happen in cases of bacterial meningitis.
Older children usually develop more specific symptoms that include fever, headaches, photophobia and neck rigidity. Older children might also develop nausea, vomiting and lethargy or irritability. Confusion can happen in patients with meningitis regardless of the involvement of the brain itself.
A positive Kernig’s sign is suggestive of bacterial meningitis in older children. During clinical examination, flexion of the hip joints while extending the knee results in back and leg pain in patients with a positive Kernig’s sign. Patients can also show a positive Brudzinski’s sign, where passive flexion of the neck can result in flexion of the hips.
Patients who develop hypertension, a slow heart rate and respiratory depression are at risk of having severe increased intracranial pressure as a complication of bacterial meningitis and require urgent medical care.
Diagnostic Workup for Bacterial Meningitis in Children
In addition to the clinical examination and history taking in the child presenting with signs suggestive of bacterial meningitis, cerebrospinal fluid analysis is perhaps the most important diagnostic test in the evaluation of such a patient. This, however, does not mean in any way that treatment with antibiotics should be delayed until the results of cerebrospinal fluid analysis are available.
Patients with bacterial meningitis usually have an increased opening pressure, more than 20 cm H2O on lumbar puncture. Additionally, the white blood cell count is usually elevated in the cerebrospinal fluid with an estimated count that is usually above 1000 x 106. Patients with bacterial meningitis usually have a low glucose concentration in the cerebrospinal fluid, < 10 mg/dL, and an elevated protein concentration, > 100 mg/dL.
A gram stain of the cerebrospinal fluid is another important test to be performed at this stage. Gram stain identification of gram-positive or gram-negative organisms is usually possible in up to 70 % of the cases. Patients with pneumococcal meningitis or meningococcal meningitis are more likely to have a positive result from their gram stain test, compared to patients infected with listeria meningitis.
The decision to perform a cerebrospinal fluid culture might be questionable. A culture is usually performed when treatment fails, but, in most cases, once antibiotic therapy is started, the culture of cerebrospinal fluid will most likely be negative. In that case, a polymerase chain reaction test might be more suitable to detect the organism’s DNA, despite low bacterial counts in the cerebrospinal fluid. The availability of polymerase chain reaction test in the clinical practice is still limited.
Treatment of Bacterial Meningitis in Children
Antibiotic therapy is very important and should be started immediately once the diagnosis of bacterial meningitis is suspected. The empirical choice of antibiotics is age dependent.

Ampicillin
Neonates should receive ampicillin plus gentamicin to cover gram-negative bacilli, listeria monocytogenes and group b streptococci. Infants aged 1 to 3 months should receive ampicillin plus cefotaxime or ceftriaxone or vancomycin. Finally, those aged above 3 months should receive cefotaxime or ceftriaxone plus vancomycin. All antimicrobial therapy should be initiated before the availability of cerebrospinal fluid test results and should be administered via the intravenous route.
In addition to antibiotic therapy, adjunctive treatment with dexamethasone is usually indicated to prevent possible complications of meningitis, such as hearing loss, developmental delay or cerebral palsy and mental retardation.
Dexamethasone, a corticosteroid, should be given before or right after the administration of the first dose of antibiotics. Dexamethasone has been proven to lower the risk of hearing loss in Haemophilus meningitis, and is believed to have a similar effect in other etiologies of meningitis.

Image: by Lecturio
Another possible adjunctive treatment for bacterial meningitis is oral glycerol. Oral glycerol was found in one study to be effective in lowering the rate of neurological sequelae after bacterial meningitis. Glycerol is cheaper and more readily available in resource-limited countries that also have a higher incidence of bacterial meningitis.



{kind=link}
{kind=link}
{kind=link}
Comentários
Enviar um comentário